48uep6bbphidcol2|ID
48uep6bbphidvals|1726
48uep6bbph|2000F98CTab_Articles|Fulltext
Primary biliary cirrhosis (PBC) is a rare causeof chronic liver disease. Anti-mitochondrial antibody (AMA)-negative PBC (5% to 8% of all PBCs) is a term designated to those patients who clinically, biochemically and histologically appear to have the classical features of PBC but are found to be negative for AMA by immunofluorescence or immunoblotting techniques. Earlier, the term auto immune cholangiopathy was used to describe this entity but current consensus holds that there is practically no difference between AMA positive and AMA negative PBC. There are very few case reports and case series of AMA-negative PBC in literature and the entity is rarer still among males .
Case Report
A 28-year old male patient presented with complaints of generalized fatigue for 2 months and itching for one month. The patient also had recurrent episodes of jaundice over the last 2 months but had no history of abdominal distension or bleeding from the upper gastrointestinal tract. Per abdominal examination revealed only mild splenomegaly without any evidence of ascites or hepatomegaly.
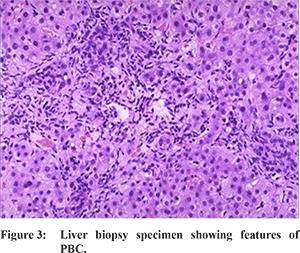
Liver function tests revealed serum bilirubin : 2.1 mg%, AST/ALT- 160/106 IU, ALP-517 IU,T.protein/serum albumin - 6.8/3. The viral markers HBsAg and Anti-HCV were negative. Tests for auto-immune markers: ANA, SMA, Anti-LKM, AMA, ANCA were negative as well. USG abdomen showed the liver with coarsened echo-texture with mild splenomegaly and no ascites. UGI endoscopy showed grade 2 oesophageal varices. MRI and MRCP abdomen revealed a cirrhotic liver with dilated portal vein, splenomegaly and minimal peri-hepatic fluid with normal biliary system and without any evidence of primary sclerosing cholangitis (PSC). (Figure 1, 2). Liver biopsy revealed multiple macroscopic nodules separated by broad fibrous septae with mixed inflammatory cell infiltrates and bile duct injury suggestive of biliary cirrhosis. (Figure 3). Testing for AMA by indirect immunofluorescence was repeated but came negative again. Immunoglobulin profile showed raised IgM levels. The patient was diagnosed with AMA-negative PBC and started on ursodeoxycholic acid (UDCA) and other conservative treatment. Subsequently, the patient improved symptomatically.
Discussion
PBC predominantly affects middle aged women and is characterised by chronic cholestasis, lymphocytic destruction of interlobular bile ducts and AMA positivity.
1 The female to male ratio is 9:1. The incidence is much lower in developing countries like India. AMA is positive in 90 to 95% cases of PBC. It is directed against E2 component of the pyruvate dehydrogenase complex (PDC-E2), the E2 unit of thebranched-chain 2-oxo-acid dehydrogenase complex (BCOADC- E2) and the E2 subunit of the 2-oxo-glutarate dehydrogenase complex (OGDC-E2).
2 These antigens are present on the inner mitochondrial membrane. The disease severity is not related to antibody titres whose levels are seen to persist even after liver transplant without disease recurrence.
ANA is present in nearly half of the cases of PBC and in up to 85% of AMA-negative PBC. Antibodies against gp210 (anti-gp210) are found in 25% of patients of AMA-positive PBC and in upto 50% of AMA negative cases. ANA with MND (multi-nuclear dots) and rim-like patterns are specific for PBC and can be considered a surrogate marker of PBC in AMA-negative cases.
2,3 PBC can be diagnosed based on biochemical and histological features as well as AMA positivity. In AMA-negative cases,other possible differentials are to be ruled out by MRCP and viral and autoimmune marker testing. The newly described antibodies to sp100 and to gp210 can be used to diagnose the disease in AMA-negative cases.
References
- Invernizzi P, Selmi C, Mackay IR, Podda M, Gershwin ME. From bases to basis: Linking genetics to causation in primary biliary cirrhosis. Clin Gastroenterol Hepatol. 2005;3:401-10.
- Prince MI, James OF. The epidemiology of primary biliary cirrhosis. Clin Liver Dis. 2003;7:795-819.
- Lacerda MA, Ludwig J, Dickson ER, Jorgensen RA, Lindor KD. Antimitochondrial antibody-negative primary biliary cirrhosis. Am J Gastroenterol. 1995;90:247-9.