|
|
|
|
 |
|
| |
 |
|
|
Case Report |
|
|
|
|
|
Keywords :
|
|
|
Biggs Saravavan Ramachandran, Mohammed Ali, Padmana Bhan P, Ganesh P, Prem Kumar, Caroline Selvi
Department Of Medical Gastroenterology,
Madras Medical College,
Park Town, Chennai 600 003, India
Corresponding Author:
Dr. Biggs Saravavan Ramachandran
Email: rbiggs21@yahoo.com
DOI:
http://dx.doi.org/
48uep6bbphidvals|475 48uep6bbph|2000F98CTab_Articles|Fulltext Frantz tumor was first described in 1959 by Frantz.[1] They account for less than 1% of pancreatic neoplasms. They are classified as borderline neoplasms (tumors of uncertain malignant potential) under WHO classification. They affect mainly young females in their teens and twenties. They are rarely seen in pediatric gastroenterology practice.
Case report
A fifteen year old female came with abdominal pain and recurrent bilious vomiting of two months duration.On examination she had right upper quadrant tenderness with otherwise normal examination findings including per rectal examination. Ultra sonogram (USG) abdomen could not delineate gall bladder separately and showed a 5 × 5 cm mass in the C loop of duodenum. Contrast enhanced computerized tomography (CECT) showed 5 × 5 cm mass within the C loop of duodenum with absence of gall bladder (Figure 1A). EUS showed a well circumscribed 5 × 5 cm mass arising from the pancreatic head through antral and duodenal windows. EUS guided FNAC showed papillary structures lined by cuboidal cells with regular nuclei and eosinophilic cytoplasm. The pathologist’s impression was a solid pseudo papillary tumor or a neuroendocrine tumor. We did immuno-histochemistry and the cells were found to be vimentin positive and cytokeratin, synaptophysin negative, suggestive of solid pseudopapillary tumor rather than a neuroendocrine tumor.
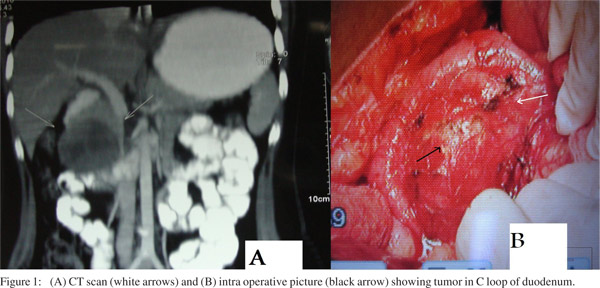
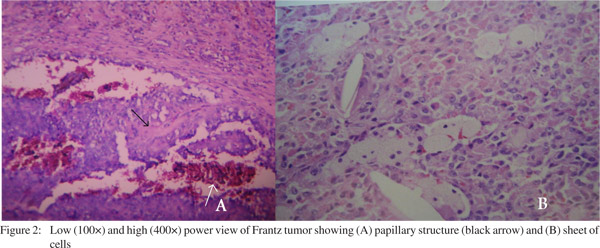 Laparotomy was done and the gall bladder was found to be absent. A pancreatic mass of size 5 × 5 cm was found in the head of pancreas (Figure 1B). The mass was enucleated and sent for histopathology. The report described a well circumscribed non-encapsulated neoplasm with extensive areas of fibrosis, necrosis, hemorrhage and inflammatory cell infiltrate. Few areas showed cystic dilated glandular spaces containing papillary processes lined by cuboidal and columnar epithelium containing oval nuclei with coarse chromatin (Figure 2A). Some areas showed solid groups of similar appearing cells (Figure 2B). Based on the above findings a diagnosis of solid pseudo papillary tumor was made. The post operative period was uneventful and the patient is doing fine after 3 months of enucleation.
Discussion
Frantz tumor or solid pseudo papillary tumor (solid cystic papillary tumor of pancreas) is a borderline tumor. It accounts for less than 1% of pancreatic tumors. Gall bladder is congenitally absent in 0.013 to 0.075% of general population.[2] So we are uncertain whether the absent gall bladder in our patient is it an incidental finding or is associated with the pseudo papillary tumor. 15% of these patients present with metastasis.[3] The treatment of choice is resection. Some surgeons prefer enucleation for small tumors.[4] Given a 5-year survival greater than 95%, radical surgery is not recommended for this neoplasm.[5] But metastatic disease may require complete surgical excision with metastatectomy.[6]
References
Laparotomy was done and the gall bladder was found to be absent. A pancreatic mass of size 5 × 5 cm was found in the head of pancreas (Figure 1B). The mass was enucleated and sent for histopathology. The report described a well circumscribed non-encapsulated neoplasm with extensive areas of fibrosis, necrosis, hemorrhage and inflammatory cell infiltrate. Few areas showed cystic dilated glandular spaces containing papillary processes lined by cuboidal and columnar epithelium containing oval nuclei with coarse chromatin (Figure 2A). Some areas showed solid groups of similar appearing cells (Figure 2B). Based on the above findings a diagnosis of solid pseudo papillary tumor was made. The post operative period was uneventful and the patient is doing fine after 3 months of enucleation.
Discussion
Frantz tumor or solid pseudo papillary tumor (solid cystic papillary tumor of pancreas) is a borderline tumor. It accounts for less than 1% of pancreatic tumors. Gall bladder is congenitally absent in 0.013 to 0.075% of general population.[2] So we are uncertain whether the absent gall bladder in our patient is it an incidental finding or is associated with the pseudo papillary tumor. 15% of these patients present with metastasis.[3] The treatment of choice is resection. Some surgeons prefer enucleation for small tumors.[4] Given a 5-year survival greater than 95%, radical surgery is not recommended for this neoplasm.[5] But metastatic disease may require complete surgical excision with metastatectomy.[6]
References
- Franz VK. Tumors of the pancreas. Atlas of tumor pathology: fasc 27–28, ser 7. Armed Forces Institute of Pathology. Washington, DC: 1959. p.32–3.
- Singh B, Satyapal KS, Moodley J, Haffejee AA. Congenital absence of the gall bladder. Surg Radiol Anat. 1999;21:221–4.
- Washington K. Solid-pseudopapillary tumor of the pancreas: challenges presented by an unusual pancreatic neoplasm. Ann Surgl Oncol. 2002;9:3–4.
- Yu PF, Hu ZH, Wang XB, Guo JM, Cheng XD, Zhang YL, et al. Solid pseudopapillary tumor of the pancreas: a review of 553 cases in Chinese literature. World J Gastroenterol. 2010;16:1209–14.
- Vollmer CM Jr, Dixon E, Grant DR. Management of a solid pseudopapillary tumor of the pancreas with liver metastases. HPB (Oxford). 2003;5:264–7.
- Martin RC, Klimstra DS, Brennan MF, Conlon KC. Solidpseudopapillary tumor of the pancreas: a surgical enigma? Ann Surg Oncol. 2002;9:35–40.
|
|
|
|
|
|