48uep6bbphidvals|455
48uep6bbph|2000F98CTab_Articles|Fulltext
Mesenteric cysts are rare intra-abdominal pathology with
prevalence 1:100,000 in adults and 1:20,000 in children.[1]
Mesenteric cysts are difficult to diagnose, and usually
asymptomatic except when complicated. Only rarely do they
present with acute intestinal obstruction.[2] We present two
cases with small bowel obstruction due to mesenteric cyst.
Both needed bowel resection with primary end-to-end
anastomosis.
Case 1
A 24-year-old female presented with history of vomiting,
constipation and abdominal distension of five days duration.
On examination, the abdomen was uniformly distended and
visible loops of small bowel were present, with no tenderness
and no palpable mass. Per rectal examination revealed an empty
non-dilated rectum. Ryle’s tube aspiration was feculent.
Abdominal radiographs showed evidence of multiple air-fluid
levels with dilated jejunal and ileal loops and no gas within the
colon. There was no free gas under the diaphragm. A diagnosis
of small bowel obstruction was made while its cause could not
be speculated.
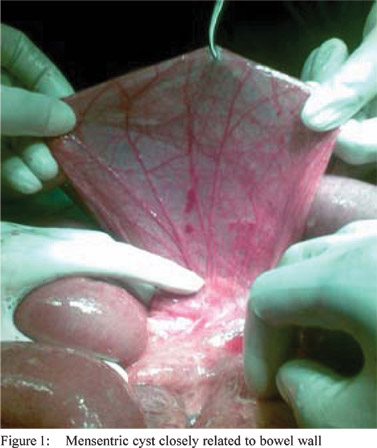
Exploratory laparotomy with midline incision was
undertaken where jejunal and ileal loop were found to be grossly
distended. A single, ruptured mesenteric cyst of 13 × 10 × 7 cm
arising from the distal ileum was found. A clockwise torsion of the cyst, leading to a constrictive narrowing of the adjacent
small bowel loop was noted. The cyst was closely related to
bowel wall with mesenteric blood vessels crossing over it, and
separation was difficult (Figure 1). Fortunately the bowel was
healthy. Hence the cyst, the mesentery containing it and the
adjacent ileum were resected and end-to-end anastomosis was
performed. Postoperative recovery was uneventful. Histology
was consistent with mesenteric cyst.
Case 2
A 44-year-old male came with complaints of vomiting and
abdominal distension of four days duration. The vomitus was
bilious with feculent smell and pain was episodic, sharp, nonradiating,
and right-sided. The patient gave a history of an
asymptomatic moving lump in abdomen since 2 years. The
abdomen was diffusely distended with no tenderness and no
palpable mass.. Abdominal radiographs showed evidence of
multiple air-fluid levels with dilated ileal loops and no gas within
the colon without free gas under the diaphragm. The diagnosis
of small bowel obstruction was made and the cause could not
be ascertained.
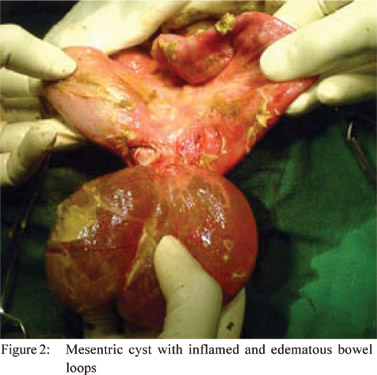
During exploratory laparotomy with midline incision, ileal
loops were found to be grossly distended. There was single
twisted, mesenteric cyst of 10 × 15 × 8 cm arising from the distal
ileum found; leading to a constrictive narrowing of the adjacent small bowel loops. The cyst was closely related to bowel wall
with inflamed and oedematous bowel loops in pool of slough
(Figure 2). Thus the cyst, the mesentery containing it and the
adjacent ileum were resected and end-to-end anastomosis was
performed. Postoperative period was uneventful. Histology
confirmed a mesenteric cyst
Discussion
Mesenteric cysts are one of the rarest abdominal pathology.[1,2] Italian anatomist Benevenni first described this entity in 1507
while performing an autopsy on an 8 years old boy.[3] Mesenteric
cysts are believed to be a manifestation of continued growth
of congenitally misplaced lymphatic tissue. The initiating event
is suspected to be a failure of the mesentery to fuse during
development. Trauma and inflammation are additional factors
implicated in their formation.[2,4] Mesenteric cysts have been
reported from the duodenal to the rectal mesentery but are
most commonly located in the ileal mesentery.[2] The cyst in our
patient was located in the mesentery of the ileum. Their
histopathological classification is based on the type of cells
present in the inner cyst wall layer. Accordingly mesenteric
cysts can be lymphatic, mesothelial, enteric, or urogenital in
origin, or derivatives of nonpancreatic pseudocysts.
Fortunately they usually behave as benign tumors, with
malignancy accounting for only 3% of the cases, arising
gradually or de novo.[2]
Patients are usually asymptomatic except when cyst gets
complicated. Symptoms are extremely variable and are related to the size and position of the cyst, with no pathognomonic
signs in the uncomplicated patients.[5] Mesenteric cysts may
cause abdominal distension or pain. They may also present
with acute symptoms secondary to complications such as
obstruction (volvulus, extrinsic compression or entrapment in
pelvis), rupture, and haemorrhage into cyst, infection or abscess
formation.[2] Infected mesenteric cyst and/or perforation are very
rare complications of a very unusual lesion. Intestinal
obstruction is a frequent complication and is usually produced
by compression of the adjacent intestine[6] as noted in our cases.
The differential diagnosis should include mesenteric cyst when
the patient presents with a history of multiple episodes of partial
small-bowel obstruction or with an asymptomatic abdominal
mass.[4]
A variety of diagnostic modalities can be used to confirm
the presence of a mesenteric cyst, but ultrasonography (USG)
and computed tomography (CT) are the best preoperative
diagnostic tools.[4] The treatment of choice is an urgent
laparotomy and complete cyst enucleation.[6] Surgical treatment
is recommended on the basis of histopathologic malignant
features and other complications, including infection of the
cyst, obstruction of adjacent bowel segment, and volvulus.[5]
But when there is a doubt of compromised bowel or its
vasculature after excision of cyst alone, segmental resection
of bowel with mesentery and cyst is preferred,[2,4] as was done
in our cases. Simple aspiration of cyst is not recommended as
it may recur. The prognosis of patients operated in a timely
manner is good with no perioperative mortality and a very low
morbidity and recurrence rate.[7]
Acknowledgments
We thank all staff members of Department of Surgery,
Jawaharlal Nehru Medical College, DMIMSU, Sawangi
(Meghe), Wardha
References
- de Perrot M, Bründler M, Tötsch M, Mentha G, Morel P.
Mesenteric cysts. Toward less confusion? Dig Surg.
2000;17:323–8.
- Christensen JA, Fuller JW, Hallock JA, Sherman RT. Mesenteric
cysts: a cause of small bowel obstruction in children. Am Surg.
1975;41:352–4.
- Braquehage J. Des kystes du mesentery. Arch Gen. 1982;170:291.
- Kurtz RJ, Heimann TM, Holt J, Beck AR. Mesenteric and
retroperitoneal Cysts. Ann Surg. 1986;203:109–12.
- Mason JE, Soper NJ, Brunt LM. Laparoscopic excision of
mesenteric cysts: a report of two cases. Surg Laparosc Endosc
Percutan Tech. 2001;11:382–4.
- Kovalivker M, Motovic A. Obstruction and gangrene of bowel
with perforation due to a mesenteric cyst in a newborn. J Pediatr
Surg. 1987;22:377–8.
- Iuchtman M, Soimu U, Amar M. Peritonitis caused by a ruptured
infected mesenteric cyst. J Clin Gastroenterol. 2001;32:452–3.