mirtazapine dosage mirtazapine side effects go
Department of Pediatric Gastroenterology,
Sanjay Gandhi Postgraduate Institute of Medical Sciences,
Lucknow - 226014, India
Corresponding Author:
Dr. Ujjal Poddar
Email: ujjalpoddar@hotmail.com
48uep6bbphidvals|650 48uep6bbph|2000F98CTab_Articles|Fulltext Ascites in childhood can have several etiologies.[1] Common causes include hepatobiliary, gastrointestinal, cardiac and genitourinary conditions. We present here an unusual case of urinary ascites in a child. To the best of our knowledge this is the first case of urinary ascites reported from India.
Case report
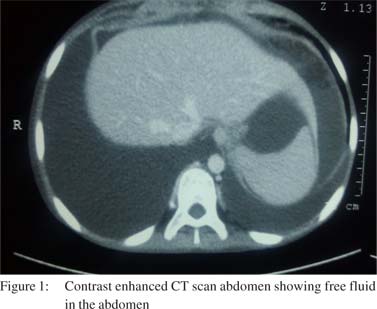
A 14-year-old girl presented with the history of pain and progressive distension of abdomen for seven days. The pain started in the supra-pubic region and became diffuse over the next two to three days. There was also a history of oliguria for three to four days. She gave no history of trauma or any other significant medical history. On examination, her vitals were stable and she had a diffusely distended, tense abdomen with fluid thrill. An erect X–ray abdomen did not reveal any air-fluid level or free peritoneal air. A CT-scan of the abdomen showed gross ascites (Figure 1). Her serum creatinine was 2.6 mg/dL. Ascitic fluid examination revealed 20 cells/mm3, all lymphocytes, proteins 0.8 g/dL, and glucose 93 mg/dL. Urine examination showed 15 to 20 leucocytes/hpf, proteins ++ and microscopic hematuria (10 to 12 red blood cells/hpf). The deranged renal parameters were attributed to pre–renal azotemia and the child was aggressively rehydrated. However, even after 12 hours of fluid resuscitation there was no improvement in her renal parameters and urine output remained low (0.2 ml/kg/hour). Around 18 hours after admission a Foley’s catheter was inserted for proper quantification of urine output.
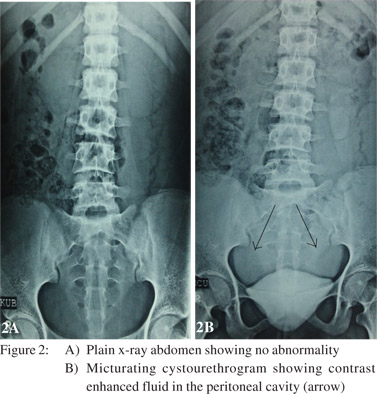
 Over the next 8 hours, the child passed around 6 liters of urine and to our surprise her abdominal distension subsided simultaneously. Serum creatinine became 0.4 mg/ dL after 24 hours. The urinary catheter was removed after 24 hours. However, within a day ascites reappeared and urine output reduced again to approximately 0.2 ml/kg/hour. This time an ascitic fluid analysis showed creatinine of 3.9 mg/dL, while simultaneous serum value was 0.4 mg/dL, suggestive of recurrent urinary ascites. A micturating cystourethrogram was performed after two days. Though it did not show a definite point of leak, there was enhancement of fluid in the peritoneal cavity suggestive of extravasation of dye from the bladder into the peritoneal cavity (Figures 2A & 2B). The child was managed conservatively by keeping the Foley’s catheter in situ and she was given intravenous cefotaxime to manage Enterococcus faecium infection detected in her urine culture. After 10 days, the Foley’s catheter was removed. Two weeks after removal of Foley’s catheter, there was no further accumulation of fluid in the peritoneal cavity and her urine output remained good.
Over the next 8 hours, the child passed around 6 liters of urine and to our surprise her abdominal distension subsided simultaneously. Serum creatinine became 0.4 mg/ dL after 24 hours. The urinary catheter was removed after 24 hours. However, within a day ascites reappeared and urine output reduced again to approximately 0.2 ml/kg/hour. This time an ascitic fluid analysis showed creatinine of 3.9 mg/dL, while simultaneous serum value was 0.4 mg/dL, suggestive of recurrent urinary ascites. A micturating cystourethrogram was performed after two days. Though it did not show a definite point of leak, there was enhancement of fluid in the peritoneal cavity suggestive of extravasation of dye from the bladder into the peritoneal cavity (Figures 2A & 2B). The child was managed conservatively by keeping the Foley’s catheter in situ and she was given intravenous cefotaxime to manage Enterococcus faecium infection detected in her urine culture. After 10 days, the Foley’s catheter was removed. Two weeks after removal of Foley’s catheter, there was no further accumulation of fluid in the peritoneal cavity and her urine output remained good.
 Discussion
Urinary ascites is an uncommon cause of ascites in children.[1] It has only been described in-utero and in neonates afflicted with congenital malformations (posterior urethral valves, bladder diverticulum), trauma and rarely spontaneous rupture of bladder.[2-5] There is no report of spontaneous rupture of the bladder in children beyond infancy. The diagnosis of urinary ascites is confirmed by an elevated ascitic fluid creatinine level relative to simultaneous serum creatinine level. An ascitic fluid/serum creatinine ratio of >1.0 is suggestive of an intraperitoneal urinary leak.[6]
Clinically bladder rupture usually presents with abdominal pain, macroscopic hematuria and an inability to void urine.7 This child had an unusual presentation of pain abdomen and ascites with no antecedent trauma and that led to the delay in diagnosis. However, once diagnosed, she improved with conservative management which has been shown to be effective in neonatal urinary ascites[3] as well as in adults with spontaneous rupture of the bladder.[7,8] The picture of oliguric acute renal failure (ARF) in the backdrop of urinary ascites is called “pseudo renal failure”, since renal function is normal but serum creatinine is elevated due to absorption through the peritoneal membrane. The rapid return of serum creatinine levels to normal with urinary drainage further distinguishes this entity from true renal failure.[8] The usual cause of bladder rupture in children includes underlying malformation or trauma but our patient suffered from spontaneous rupture of a healthy bladder. In adults, spontaneous rupture of bladder has been associated with alcohol intoxication.[8] An over distended bladder with dulled micturition sensation leads to spontaneous rupture in these patients. However, the etiology in our case remained unknown as there was no history of trauma, drugs or intoxication.
In summary, we encountered a case of urinary ascites due to spontaneous rupture of the bladder with a laboratory picture mimicking oliguric ARF. The patient improved with conservative management. Physicians should be aware of this entity as a delay in diagnosis can increase mortality and morbidity.
References
Discussion
Urinary ascites is an uncommon cause of ascites in children.[1] It has only been described in-utero and in neonates afflicted with congenital malformations (posterior urethral valves, bladder diverticulum), trauma and rarely spontaneous rupture of bladder.[2-5] There is no report of spontaneous rupture of the bladder in children beyond infancy. The diagnosis of urinary ascites is confirmed by an elevated ascitic fluid creatinine level relative to simultaneous serum creatinine level. An ascitic fluid/serum creatinine ratio of >1.0 is suggestive of an intraperitoneal urinary leak.[6]
Clinically bladder rupture usually presents with abdominal pain, macroscopic hematuria and an inability to void urine.7 This child had an unusual presentation of pain abdomen and ascites with no antecedent trauma and that led to the delay in diagnosis. However, once diagnosed, she improved with conservative management which has been shown to be effective in neonatal urinary ascites[3] as well as in adults with spontaneous rupture of the bladder.[7,8] The picture of oliguric acute renal failure (ARF) in the backdrop of urinary ascites is called “pseudo renal failure”, since renal function is normal but serum creatinine is elevated due to absorption through the peritoneal membrane. The rapid return of serum creatinine levels to normal with urinary drainage further distinguishes this entity from true renal failure.[8] The usual cause of bladder rupture in children includes underlying malformation or trauma but our patient suffered from spontaneous rupture of a healthy bladder. In adults, spontaneous rupture of bladder has been associated with alcohol intoxication.[8] An over distended bladder with dulled micturition sensation leads to spontaneous rupture in these patients. However, the etiology in our case remained unknown as there was no history of trauma, drugs or intoxication.
In summary, we encountered a case of urinary ascites due to spontaneous rupture of the bladder with a laboratory picture mimicking oliguric ARF. The patient improved with conservative management. Physicians should be aware of this entity as a delay in diagnosis can increase mortality and morbidity.
References
- Giefer MJ, Murray KF, Colletti RB. Pathophysiology, diagnosis, and management of pediatric ascites. J Pediatr Gastroenterol Nutr. 2011;52:503–13.
- Redman JF, Seibert JJ, Arnold W. Urinary ascites in children owing to extravasation of urine from the bladder. J Urol. 1979;122:409–11.
- Vasdev N, Coulthard MG, De la hunt MN, Starzyk B, Ognjanovic M, Willetts IE. Neonatal urinary ascites secondary to urinary bladder rupture. J Pediatr Urol. 2009;5:100–4.
- Kuwata T, Matsubara S, Nakamura S, Nakai H. Urinary ascites in a fetus with posterior urethral valve: antenatal diagnosis. Pediatr Int. 2011;53:281–2.
- Murphy D, Simmons M, Guiney EJ. Neonatal urinary ascites in the absence of urinary tract obstruction. J Pediatr Surg. 1978;13:529–31.
- Kato A, Yoshida K, Tsuru N, Ushiyama T, Suzuki K, Ozono S, et al. Spontaneous rupture of the urinary bladder presenting as oliguric acute renal failure. Intern Med. 2006;45:815–8.
- Saliba W, Grant ME. Conservative management of spontaneous bladder rupture. Kansas J Med. 2011;4:44–6.
- Stebbing J, Ezra DG, Cackett PD, Greenstein AS. Ascites and apparent renal failure treated with a Foley catheter. J R Soc Med. 1999;92:582–3.
|