Piyush Kumar Sinha1, Vivek Mangla1, Chhagan Behari2, Archana Rastogi2, TK Chattopdhyay1
Departments of HPB Surgery1 and Pathology,2
Institute of Liver and Biliary Sciences,
D1, Vasant Kunj, New Delhi - 110070, India
Corresponding Author:
Dr. Vivek Mangla
Email: mangla.vivek@gmail.com
48uep6bbphidvals|632 48uep6bbph|2000F98CTab_Articles|Fulltext Lymphoepithelioma-like carcinoma (LLC) of the biliary tract is a relatively recently recognized entity. LLC involving the gall bladder (LLC-GB) has been described only once in the literature.[1]
Case report
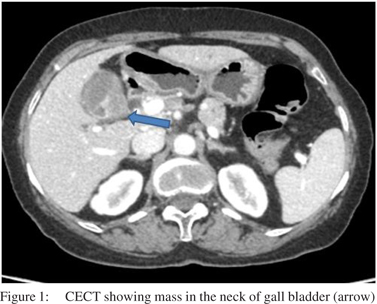
A 64-year-old lady presented with right upper abdominal pain of three months duration. Clinical examination was normal. CT scan (Figure 1) revealed a 2.4×2.0×3.1 cm heterogeneously enhancing soft tissue lesion arising in relation to the gall bladder neck. The common bile duct was dilated (10 mm) till its lower end with no evidence of obstruction at the ampulla.
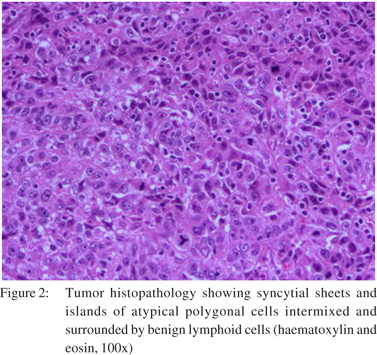
Subcentimetric lymph nodes were present in the hepatoduodenal ligament. A provisional diagnosis of carcinoma gall bladder was made and the patient was taken up for surgery. At surgery, there was a 3 cm mass arising from the gallbladder neck and confined to the gall bladder. There were no peritoneal or liver metastases. Extended cholecystectomy was performed. Cystic duct margin was free of tumor on frozen section analysis. The postoperative course was uneventful and the patient was discharged in satisfactory condition. Histopathology of the resected specimen showed surface epithelial ulceration and infiltration by a tumor composed of syncytial sheets and islands of atypical polygonal cells intermixed and surrounded by lymphoid cells (Figure 2). The tumor had infiltrated the mucosa, muscularis propria and had reached up to the subserosa. Perineural invasion was seen but there was no lymphovascular invasion. Cystic duct margin, liver transection margin and all resected lymph nodes were free of tumour. Tumour cells showed positive cytoplasmic staining with pancytokeratin and were for negative for Epstein-Barr virus on immunohistochemistry. Patient has been followed up for 18 months after surgery with no evidence of recurrence.
 Discussion
Schmincke in 1921 described a distinct type of undifferentiated nasopharyngeal carcinoma where tumor cells grow in a diffuse manner mimicking a malignant lymphoma.[2] This tumor has been designated as lymphoepithelial carcinoma or undifferentiated carcinoma with lymphocytic stroma. Several studies have reported the presence of similar tumor in several extrapharyngeal sites such as lungs, stomach, salivary glands and thymus.[3] There are multiple recent case reports describing lymphoepithelioma-like carcinoma (LLC) of the biliary tract with intra-hepatic bile duct being the most common site of origin.[2] To the best of our knowledge, only two cases of extrahepatic LLC have been reported, one in the gall bladder and another in the distal bile duct.[1,4] Extra-nasopharyngeal LLC are also associated with EBV infection.[2] The prognosis of biliary tract LLC is generally considered better than adenocarcinoma.[5] This case has been reported for its rarity and lack of association with EBV infection.
References
Discussion
Schmincke in 1921 described a distinct type of undifferentiated nasopharyngeal carcinoma where tumor cells grow in a diffuse manner mimicking a malignant lymphoma.[2] This tumor has been designated as lymphoepithelial carcinoma or undifferentiated carcinoma with lymphocytic stroma. Several studies have reported the presence of similar tumor in several extrapharyngeal sites such as lungs, stomach, salivary glands and thymus.[3] There are multiple recent case reports describing lymphoepithelioma-like carcinoma (LLC) of the biliary tract with intra-hepatic bile duct being the most common site of origin.[2] To the best of our knowledge, only two cases of extrahepatic LLC have been reported, one in the gall bladder and another in the distal bile duct.[1,4] Extra-nasopharyngeal LLC are also associated with EBV infection.[2] The prognosis of biliary tract LLC is generally considered better than adenocarcinoma.[5] This case has been reported for its rarity and lack of association with EBV infection.
References
- Todd DL, Ro JY, Gully LM, Ayala AG. Lymphoepitheliomalike carcinoma of the gallbladder. Int J Surg Pathol. 1996;4:183-7.
- Schmincke A. Uber lymphoepitheliale geschwulste. Beitr pathol. Anat Allg Pathol. 1921;68:161–70.
- Iezzoni JC, Gaffey MJ, Weiss LM. The role of Epstein-Barr virus in lymphoepithelioma-like carcinomas. Am J Clin Pathol. 1995;103:308–15.
- Ishida M, Mori T, Shiomi H, Naka S, Tsujikawa T, Andoh A, et al. Non-Epstein-Barr virus associated lymphoepithelioma-like carcinoma of the inferior common bile duct. World J Gastrointest Oncol. 2011;3:111–5.
- Henderson-Jackson E, Nasir NA, Hakam A, Nasir A, Coppola D. Primary mixed lymphoepithelioma-like carcinoma and intrahepatic cholangiocarcinoma: a case report and review of literature. Int J Clin Exp Pathol. 2010;3:736–41.
|