48uep6bbphidvals|561
48uep6bbph|2000F98CTab_Articles|Fulltext
Persistence of congenital esophagobronchial fistulae into adulthood is rare.[1] They usually present in infants and may occur with or without esophageal atresia.[2]
Case report
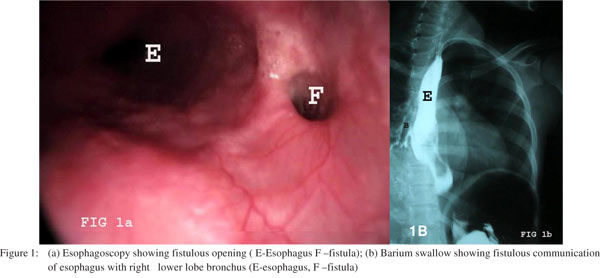
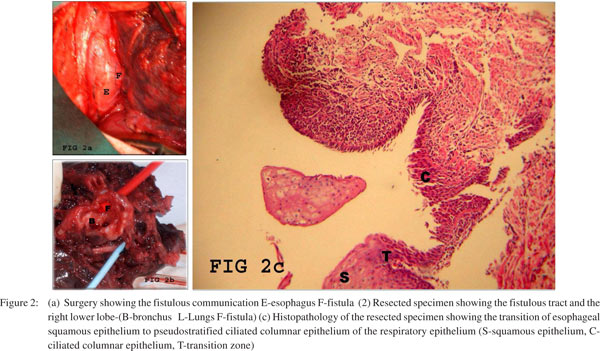
A 20 yr old female presented with history of recurrent respiratory infection from the age of 13 years. At presentation, she had history of prolonged cough soon after food intake which was more with liquid food for the last 3 years. There was no past history of any surgery, trauma, tuberculosis or any other major illness. On examination, she was moderately built and poorly nourished. Respiratory system examination revealed coarse crepitations in the right lower lobe areas. Routine blood investigations were normal. Esophagogastroduodenoscopy showed a opening in the esophagus 30 cm from the incisor tooth (Figure 1a). Barium swallow showed spill over of barium from the esophagus into the right lower bronchus (Figure 1b). CT scan showed communication between esophagus and right lower bronchus and destruction of the right lower lobe with bronchiectatic changes. Bronchoscopy showed right posterior basal segmental orifice located more an teriorly with plenty of secretions. During surgery a fistulous communication between the esophagus and the bronchus (Figure 2a) noted. Fistula along with the right lower lobe was resected. Resected specimen (Figure 2b) was sent for histopathological analysis. The esophageal squamous epithelium was seen to merge with the pseudostratified ciliated columnar epithelium of the respiratory tract (Figure 2c). Patient had an uneventful recovery during the post operative period and is currently under follow up. She has not developed further respiratory infection and is asymptomatic now.
Discussion
Benign bronchoesophageal fistulas can remain undiagnosed for years. Bouts of coughing when swallowing liquids (Ohno’s sign) are reported to be pathognomonic for this condition and present in 65% of cases.[3,4] The congenital nature of the fistula is suggested by the absence of adherent lymph nodes, past or present surrounding inflammation, by the presence of a mucosa and definitive muscularis mucosa within the fistulous tract.[5] Braimbridge and Keith[6] classified congenital bronchoesophageal fistulas into four types:
- Type I - fistula is associated with an esophageal diverticulum.
- Type II - short tract running directly from the esophagus to the bronchus.
- Type III - fistula communicates between the esophagus and a cyst in the lung lobe
- Type IV - fistula between the esophagus and a sequestered pulmonary segment.
- Type II is the most prevalent and comprises almost 90% of all cases in some series. Our patient had a simple type a! fistula.
The insidious nature of fistula may become life threatening, with repeated infections leading to pneumonia, bronchiectasis and abscess formation.[7] Despite, the benign nature of this anomaly, if left untreated, it may lead to fatal complications. For most cases of fistula formation, surgical management via thoracotomy is the traditional treatment. The fistula is exposed and divided, and both the defects in the bronchus and the esophagus are repaired with interposition of viable tissue (e.g., pleural or muscular flap) between the suture lines. Pulmonary resection is often needed in patients with coexistent pulmonary disease. The prognosis after surgical repair is excellent. Obliteration of the esophageal orifice with silver nitrate or biological glue is reserved for the patient who cannot tolerate thoracotomy.[8]
References
- Freixinet J, Rami R, Ledo R, Corbal M, Calzadilla G, Sánchez- Lloret J Congenital bronchoesophageal fistula in adults. Report of three cases. Eur J Cardiothorac Surg. 1990;4:451–3.
- Smith BD Jr, Mikaelian DO, Cohn HE Congenital bronchoesophageal fistula in the adult. Ann Otol Rhinol Laryngol. 1987;96:65–7.
- Linnane BM, Canny G. Congenital broncho-esophageal fistula: A case report. Respir Med. 2006;100:1855–7.
- Kim JH, Park KH, Sung SW, Rho JR. Congenital bronchoesophageal fistulas in adult patients. Ann Thorac Surg. 1995;60:151–5.
- Ramo OJ, Salo JA, Mattila SP. Congenital bronchoesophageal fistula in the adult. Ann Thorac Surg. 1995;59:887–9; discussion 890.
- Braimbridge MV, Keith HI. Oesophago-bronchial fistula in the adult. Thorax. 1965;20:226–33.
- Zach MS, Eber E. Adult outcome of congenital lower respiratory tract malformations. Thorax. 2001;56:65–72.
- Su L, Wei XQ, Zhi XY, Xu QS, Ma T. Congenital bronchoesophageal fistula in an adult: a case report. World J Gastroenterol. 2007;13:3776–7.