48uep6bbphidvals|557
48uep6bbph|2000F98CTab_Articles|Fulltext
Pancreatic anomalies are only rarely reported, but complete agenesis of the dorsal pancreas is extremely rare.[1] Partial agenesis mostly affects dorsal part, because it relies on different genes and signaling events from those of ventral pancreas.[2] Our case presented with recurrent episodes of pancreatitis.
Investigations showed absent body and tail of the pancreas. Patient had no evidence of chronicity in the remaining pancreas.
Case report
A 27yr old male patient presented with history of abdominal pain in the epigastrium for the last two years. He had recurrent episodes of pain which used to increase with food intake. Twice he had severe pain which required admission to the hospital. He used to note that there is increase in pain after bouts of alcohol intake. The pain used to radiate to the back and last for hours. There was no history of trauma in the past. General examination was non contributory. Abdomen was soft and did not reveal any mass or free fluid.
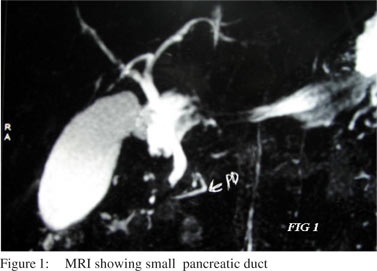
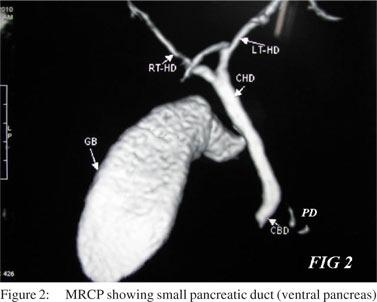
His routine investigations were normal. Amylase and lipase levels were normal at presentation. His blood sugar and serum calcium were normal. His glucose tolerance test was normal. Triglyceride levels were normal. Ultrasound report showed bulky pancreatic head.. Even though he had significant history of alcohol intake, a CT scan was advised to rule out any structural abnormality. CT scan showed absence of body and tail of pancreas. MRI (Figure 1) and MRCP (Figure 2) showed complete absence of body and tail of pancreas (which develops from dorsal pancreatic bud). There was no evidence of calcification or pancreatic duct dilatation.
 He was advised to stop alcohol and was put on pancreatic enzymes. He is under follow up now. For the last six months he never had any abdominal pain. He is planned for sphincterotomy of pancreatic duct if he further develops recurrent pancreatitis, as there are occasional case reports of pain relief with pancreatic sphincterotomy.[3]
Aplasia, or varying degrees of hypoplasia, of the pancreas were classified histologically by Lumb et al[4] into (1) complete (2) partial (a) involving both endocrine and exocrine tissue (b) involving endocrine tissue only (c) involving exocrine tissue only. According to the degree of immaturity of the dorsal pancreas development, hypoplasia of the pancreas is classified clinically into three types (1) total agenesis of the dorsal pancreas (2) hypogenesis of the body and tail (3) hypogenesis of the tail. In type 1, the major pancreatic duct can be identified on endoscopic retrograde cholangiopancraphy (ERCP) images, but not the minor pancreatic duct. In types 2 and 3, ERCP images show both major and minor pancreatic ducts communicating with each other.
Our patient had type 1 total agenesis of dorsal pancreas, as MRCP was showing only part of major pancreatic duct in the ventral bud of pancreas. There was no evidence of any chronic pancreatitis.
The etiology of the abdominal pain of congenital abnormality of the pancreas is unknown and has been presumed to be due to pancreatitis or autonomic neuropathy similar to that in patients with diabetes mellitus.[5]
He was advised to stop alcohol and was put on pancreatic enzymes. He is under follow up now. For the last six months he never had any abdominal pain. He is planned for sphincterotomy of pancreatic duct if he further develops recurrent pancreatitis, as there are occasional case reports of pain relief with pancreatic sphincterotomy.[3]
Aplasia, or varying degrees of hypoplasia, of the pancreas were classified histologically by Lumb et al[4] into (1) complete (2) partial (a) involving both endocrine and exocrine tissue (b) involving endocrine tissue only (c) involving exocrine tissue only. According to the degree of immaturity of the dorsal pancreas development, hypoplasia of the pancreas is classified clinically into three types (1) total agenesis of the dorsal pancreas (2) hypogenesis of the body and tail (3) hypogenesis of the tail. In type 1, the major pancreatic duct can be identified on endoscopic retrograde cholangiopancraphy (ERCP) images, but not the minor pancreatic duct. In types 2 and 3, ERCP images show both major and minor pancreatic ducts communicating with each other.
Our patient had type 1 total agenesis of dorsal pancreas, as MRCP was showing only part of major pancreatic duct in the ventral bud of pancreas. There was no evidence of any chronic pancreatitis.
The etiology of the abdominal pain of congenital abnormality of the pancreas is unknown and has been presumed to be due to pancreatitis or autonomic neuropathy similar to that in patients with diabetes mellitus.[5]
Diabetes was present in most of the reported cases. In some cases it substantially preceded the onset of abdominal discomfort and the diagnosis.[6] Most patients with congenital short pancreas with normal situs had diabetes mellitus and were o,occasionally associated with pancreatitis.
References
- Fukuoka K, Ajiki T, Yamamoto M, Fujiwara H, Onoyama H, Fujita T, et al. Complete agenesis of the dorsal pancreas. J Hepatobiliary Pancreat Surg. 1999;6:94–7.
- Johansson KA, Grapin-Botton A. Development and diseases of the pancreas. Clin Genet. 2002;62:14–23.
- Bretagne JF, Darnault P, Raoul JL, Gardon Y, Gosselin M, Cousin P, et al. Calcifying pancreatitis of a congenital short pancreas: a case report with successful endoscopic papillotomy. Am J Gastroenterol. 1987;82:1314–7.
- Lumb G, Beautyman W. Hypoplasia of the exocrine tissue of the pancreas. J Pathol Bacteriol. 1952; 64:679–86.
- Gilinsky NH, Del Favero G, Cotton PB, Lees WR. Congenital short pancreas: a report of two cases. Gut. 1985;26:304–10.
- Morita M, Otsubo C, Kozu T, Shibata I, Toki F, Oi I, et al. Aplasia of the body and tail of the pancreas—a report of two cases (article in Japanese). Nihon Shokakibyo Gakkai Zasshi. 1980;77:102–6.