Sangeetha Siva, N. Satish, H.V. Shivaram
Department of General Surgery,
St. Philomenas Hospital, Mother Teresa Road,
Bangalore, India
Corresponding Author:
Dr. H.V. Shivaram
Email: hvshivaram@gmail.com
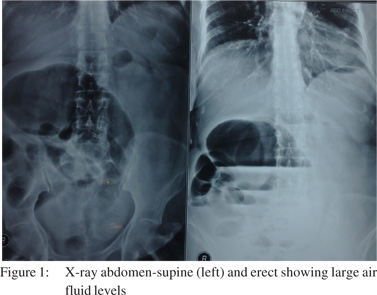
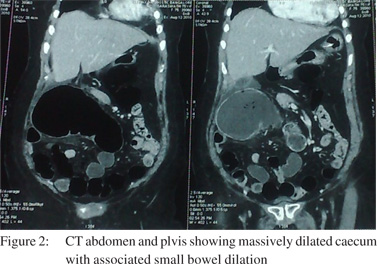
48uep6bbphidvals|542 48uep6bbph|2000F98CTab_Articles|Fulltext Caecal volvulus is a rare clinical condition causing intestinal obstruction. It is responsible for 1% of all adult intestinal obstructions and 30% of all cases of volvulus involving the colon. The most common signs associated with it are abdominal pain, constipation and vomiting; none of which are specific for the condition.[1] Abdominal radiography permits diagnosis in 70% of cases by 3 typical signs: caecum dilatation, a single air–fluid level in the right lower quadrant, and absence of gas in the colon.[2] The CT scan typically shows a massively dilated caecum with associated small bowel dilation. The twisted or “whirl” mesenteric configuration around the ileocolic artery is pathognomonic of axial caecal volvulus. Overall, radiographic studies confirm the diagnosis of caecal volvulus 90% of the time. The remainder are diagnosed at surgery.[3] In this report we present the case of a 70-year-old woman with caecal volvulus.
Case report
A 70-year-old woman presented with acute pain abdomen, vomiting and constipation since one day. The pain was diffuse and colicky in nature. She had no co-morbid illness and no history of surgery in the past.
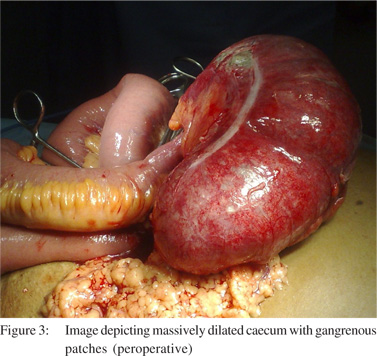
X-ray abdomen (erect and supine) (Figure 1) showed a loop of dilated large bowel on the right side with multiple loops of dilated small bowel showing air fluid levels. CT abdomenand pelvis (Figure 2) revealed a large caecal volvulus with an obstructed proximal bowel and a decompressed distal colon with malrotation of the gut. An emergency laparotomy was performed which confirmed the presence of caecal volvulus and malrotation of the gut. The caecum was massively dilated with a few gangrenous patches (Figure 3). Detorsion and a right hemicolectomy with primary anastomosis using a stapler was performed. The post-operative recovery was uneventful and the patient was discharged after 8 days.
 Discussion
Patients with volvulus are commonly elderly, debilitated, and bedridden. It has also been postulated that postsurgical adhesions contribute to the formation of fixation points, thus promoting volvulus development. Other conditions, such as late-term pregnancy, high-fiber intake, adynamic ileus, chronic constipation, and distant colon obstruction, have also been implicated in caecal volvulus.[2] It is imperative to distinguish a caecal volvulus from a sigmoid volvulus. Caecal volvulus is more common in women, rotates in a clockwise direction, and is best treated by primary right colectomy. Sigmoid volvulus
on the other hand, is more common in men, rotates in a counterclockwise direction, and is often treated by intubation through the sigmoidoscope.[4-5]
Rapid diagnosis, resuscitation and surgery are imperative as the mortality rate in gangrenous caecal volvulus is 17-40%.[6] Surgery is the treatment of choice and intervention is advised as soon as the diagnosis is made. Ileocolic resection without detorsion (eventually with pexy of the remnant colon) is the standard treatment and offers a low mortality rate with zero recurrence. Other contemporary surgical options include manual detorsion, caecopexy, caecostomy, and colectomy by open or laparoscopic approaches.[7] Attempts at reduction by colonoscopy or barium enema are anecdotal methods with a risk of dangerous delay before surgery.
References
Discussion
Patients with volvulus are commonly elderly, debilitated, and bedridden. It has also been postulated that postsurgical adhesions contribute to the formation of fixation points, thus promoting volvulus development. Other conditions, such as late-term pregnancy, high-fiber intake, adynamic ileus, chronic constipation, and distant colon obstruction, have also been implicated in caecal volvulus.[2] It is imperative to distinguish a caecal volvulus from a sigmoid volvulus. Caecal volvulus is more common in women, rotates in a clockwise direction, and is best treated by primary right colectomy. Sigmoid volvulus
on the other hand, is more common in men, rotates in a counterclockwise direction, and is often treated by intubation through the sigmoidoscope.[4-5]
Rapid diagnosis, resuscitation and surgery are imperative as the mortality rate in gangrenous caecal volvulus is 17-40%.[6] Surgery is the treatment of choice and intervention is advised as soon as the diagnosis is made. Ileocolic resection without detorsion (eventually with pexy of the remnant colon) is the standard treatment and offers a low mortality rate with zero recurrence. Other contemporary surgical options include manual detorsion, caecopexy, caecostomy, and colectomy by open or laparoscopic approaches.[7] Attempts at reduction by colonoscopy or barium enema are anecdotal methods with a risk of dangerous delay before surgery.
References
- Consorti ET, Liu TH. Diagnosis and treatment of caecal volvulus. Postgrad Med J. 2005;81:772–6.
- Habre J, Sautot-Vial N, Marcotte C, Benchimol D. Caecal volvulus. Am J Surg. 2008;196:e48–9.
- Pulvirenti E, Palmieri L, Toro A, Di Carlo I. Is laparotomy the unavoidable step to diagnose caecal volvulus? Ann R Coll Surg Engl. 2010;92:W27–9.
- Hiltunen KM, Syrja H, Matikainen M. Colonic volvulus. Diagnosis and results of treatment in 82 patients. Eur J Surg. 1992;158:607–11.
- Meyers JR, Heifetz CJ, Baue AE. Cecal volvulus: a lesion requiring resection. Arch Surg. 1972;104:594–9.
- Joosse P, Vrouenraets BC, Scholten P, van Tets WF, Steller EP. Colonic obstruction due to volvulus of the sigmoid colon or caecum. Ned Tijdschr Geneeskd. 2010;154:A863.
- Ruiz-Tovar J, Calero Garcia P, Morales Castineiras V, Martinez Molina E. Caecal volvulus: presentation of 18 cases and review of literature. Cir Esp. 2009;85:110–3.
|