Mukund A1, Gamanagatti S1, Saraya A2
Department of Radiology,1
Department of Gastroenterology,2
All India Institute of Medical Sciences,
New Delhi - 110029, India
Corresponding Author:
Dr. Shivanand Gamanagatti
Email: shiv223@rediffmail.com
48uep6bbphidvals|481 48uep6bbph|2000F98CTab_Articles|Fulltext Pancreatitis is an inflammatory disease of pancreas which may lead to a variety of vascular complications. Common complications are hemorrhage into a pseudocyst, erosion of arteries adjacent to inflamed pancreas leading to frank intraperitoneal bleed or pseudoaneurysm formation and thrombosis of the portal venous system.[1] Inferior vena cava (IVC) thrombosis is a very rare condition associated with pancreatitis and only few case reports are there in the literature describing this condition.[2,3,4,5] Here we report a case of chronic pancreatitis having IVC thrombus extending into bilateral renal veins.
Case Report
A 35 year old man, known alcoholic, with previous episode of acute pancreatitis 5 years back presented with acute abdomen to the casualty. The patient gave history of similar episodes in the past; however the pain was never as severe as he had this time. On examination the abdomen was distended and tender with presence of guarding and rigidity. He had mild tachycardia but blood pressure was normal. Blood examination revealed mildly elevated serum amylase level. Based on history and clinical findings, a diagnosis of acute on chronic pancreatitis was made and contrast enhanced CT scan of abdomen was advised.
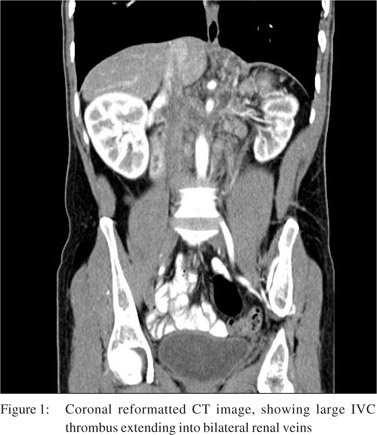
The CT scan showed the pancreas to be mildly atrophic with a dilated main pancreatic duct consistent with chronic pancreatitis. No parenchymal calcification or intraductal calculi were seen. An unusual finding noted was a large intraluminal thrombus within the IVC extending from the level of renal hilum up to the intahepatic IVC (Figure 1). The thrombus was also seen extending into bilateral renal veins. Celiac artery and its branches were normal in course and caliber. The spleno-portal axis was also normal. Based on imaging a diagnosis of chronic pancreatitis with large IVC thrombus extending into bilateral renal veins was made.
Discussion
Vascular complications in pancreatitis are well documented. Nearly one fourth of patients having pancreatitis may develop vascular complications. Hemorrhage being one of the most common and most dreaded complications associated with it.[6] Formation of pseudoaneurysms secondary to pancreatitis is well known.[7] Pseudoaneurysms form due to adjacent inflammation necrotizing the vessel wall or due to release of pancreatic enzymes eroding the vessel. Another vascular complication associated with pancreatitis is thrombosis of spleno-portal axis. However splenic vein thrombosis is more common and may occur in about 10 - 40% of patients with chronic pancreatitis.[8]
IVC thrombosis is commonly seen as an extension of deep vein thrombosis (DVT). However, a variety of causes may lead to this condition. Important ones include renal cell carcinoma (RCC) and retroperitoneal tumors. Extrinsic compression may also lead to this condition, like compression produced by aneurysms, abscesses, cysts, hematoma and or any dysfunction in coagulation system. Urgent management is required for this condition as it may further lead to pulmonary embolism. Standard treatment for DVT and IVC thrombosis remains systemic anticoagulation, however mechanical interruption of the pathway may be offered to patients who have contraindication for anticoagulation by placing an IVC filter.
Association of IVC thrombosis in chronic pancreatitis is less known. Only few case reports are there in the literature describing this entity. The present case is one among them presenting with the unusual complication of IVC thrombosis extending into bilateral renal veins. The patient did not had lower limb edema or abdominal collaterals despite having a large IVC thrombus extending from the level of renal hilum to intrahepatic IVC, ending below the confluence of hepatic veins.
The pathogenesis of IVC thrombosis in pancreatitis is not well understood but the factors contributing to the formation of IVC thrombus are likely to be similar as of spleno-portal thrombosis. The possible factors include: inflammation, edema and cellular infiltration adjacent to IVC; mass effect and compression due to pseudocyst or bulky/calcified pancreas; intimal injury caused by acute pancreatitis or recurrent episodes of pancreatitis. It is a difficult question to answer whether the thrombus originated in the IVC and extended below to involve bilateral renal veins or it formed in renal veins and extended to involve the IVC. However the authors believe that the thrombus formed in IVC due to adjacent inflammatory changes and intimal injury caused by recurrent episodes of pancreatitis and extended further to involve bilateral renal veins.
References
- Mallick IH, Winslet MC. Vascular complications of pancreatitis. JOP. 2004;5:328–37.
- Ma SK, Kim SW, Kim NH, Choi KC. Renal vein and inferior vena cava thrombosis associated with acute pancreatitis. Nephron. 2002;92:475–7.
- Ohta H, Hachiya T. A case of inferior vena cava thrombosis and pulmonary embolism secondary to acute exacerbation of chronic pancreatitis: a rare finding in radionuclide venography. Ann Nucl Med. 2002;16:147–9.
- Jones AL, Ojar D, Redhead D, Proudfoot AT. Case report: Use of an IVC filter in the management of IVC thrombosis occurring as a complication of acute pancreatitis. Clin Radiol. 1998;53:462–4.
- Ohno T, Takabayashi A, Maki A, Usui Y, Takeuchi K, Kohno S. Complete obstruction of the inferior vena cava due to chronic relapsing pancreatitis: a case report. Nippon Geka Hokan. 1994;63:215–20.
- Vujic I. Vascular complications of pancreatitis. Radiol Clin North Am. 1989;27:81–91.
- Carr JA, Cho JS, Shepard AD, Nypaver TJ, Reddy DJ. Visceral pseudoaneurysms due to pancreatic pseudocysts: rare but lethal complications of pancreatitis. J Vasc Surg. 2000;32:722–30.
- Bernades P, Baetz A, Levy P, Belghiti J, Menu Y, Fekete F. Splenic and portal venous obstruction in chronic pancreatitis. A prospective longitudinal study of a medical-surgical series of 266 patients. Dig Dis Sci. 1992;37:340–6.
|