Shailendra Lalwani, Manoj Gupta, Vibha Varma, Naimish Mehta, Vinay Kumaran, Samiran Nundy
Department of Surgical
Gastroenterology and Liver Transplantation,
Sir Ganga Ram Hospital,
New Delhi – 110060, India
Corresponding Author:
Dr. Shailendra Lalwani
Email: slalwani2008@yahoo.com
Abstract
Background/Aim: Late presentation of small bowel strictures following blunt abdominal trauma is rather uncommon and there have been few previous reports of its occurrence. Most patients with blunt abdominal trauma without perforation or major bleeding are managed conservatively, making the diagnosis of less conspicuous intestinal injuries difficult.
Methods: We reviewed our prospectively maintained surgical records over a period of 12 years and found that 8 patients developed small bowel obstruction subsequent to a history of blunt trauma abdomen which had been initially managed conservatively.
Results: A total of 7 males and 1 female with a mean age of 37 (range 23 - 48) years were examined in this study. The most common presentation was pain and vomiting with abdominal distension, noted in 5 patients; but three patients presented only with abdominal pain. The strictures were solitary in all cases, with the most common site being the terminal ileum. The average interval between the trauma and presentation of small bowel obstruction was 138 (range 7 to 550) days. Barium meal studies and computerized tomography were used to establish the diagnosis and laparotomy with resection of the involved bowel was curative. There was no mortality.
Conclusions: Post traumatic small bowel obstruction should be kept in the differential diagnosis of patients who presented with abdominal pain, sometimes without distension and vomiting, and who have a history of blunt trauma abdomen.
|
48uep6bbphidvals|469 48uep6bbph|2000F98CTab_Articles|Fulltext Patients with blunt abdominal trauma are often managed without surgical intervention, if there are no signs of bowel perforation or hypovolemic shock due to blood loss.
Consequently, mesenteric injuries and small bowel haematoma may go undiagnosed.[1] There are only a few reports highlighting such cases, with no more than four reported cases of small bowel stricture following abdominal trauma, which manifested as early as one week or as late as twenty six years after the injury.[2,3] We present our experience of eight such patients.
Methods
We retrospectively identified and examined from our prospectively maintained database, eight consecutive patients with post traumatic small bowel stricture that were admitted to our department at the Sir Ganga Ram Hospital, New Delhi, between August 1996 and July 2008.
All 8 patients presented with signs and symptoms of small intestinal obstruction and a past history of road traffic accident during which they had sustained blunt abdominal trauma,which had been managed conservatively. The diagnosis of a post traumatic stricture was based on prior history of blunt abdominal trauma, barium studies, computed tomography of the bowel, the findings at surgery and a histopathology report of an ischaemic lesion. The data examined included patient demographics and time interval between the trauma and the appearance of symptoms of intestinal obstruction.
Results
The patients were aged between 23 and 48 (mean 37) years with a male:female ratio of 7:1. All patients presented with abdominal pain and vomiting and recurrent abdominal distension was reported in only five patients.
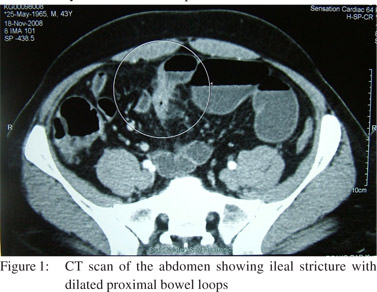
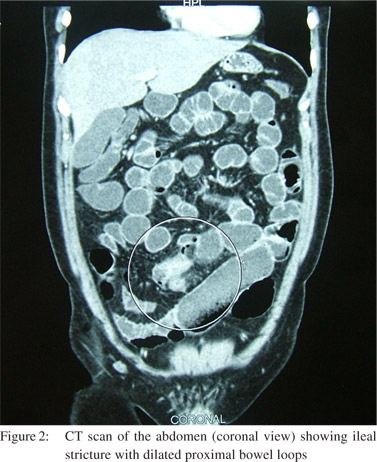
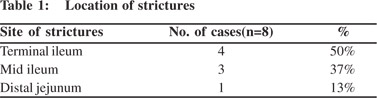
The diagnosis of small bowel stricture was primarily based on radiography utilizing plain X-ray abdomen and barium meal studies. An additional CT scan with contrast was performed when the diagnosis was not confirmed by above modalities (Figure 1-3). After experience of the first case, all following cases were correctly diagnosed with post traumatic stricture pre-operatively, with confirmation of the diagnosis during surgery. Strictures in small bowel were found to be solitary in all the cases, with the most common site being the terminal ileum. The number and sites of strictures are summarized in Table 1.
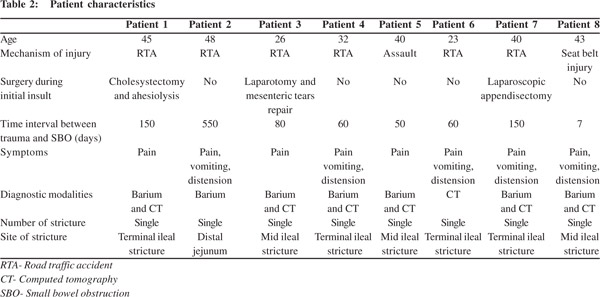
All the patients had a history of prior hospitalization immediately after the initial episode of trauma. Five of them were treated conservatively at the initial admission. Three patients underwent surgery with one patient undergoing a laparotomy with repair of a mesenteric tear, the second patient undergoing a diagnostic laparoscopy and appendicectomy and the third underwent adhesiolysis and cholecystectomy. In none of these three cases was an intestinal procedure performed.The average time between the initial trauma and presentation of small bowel obstruction was 138 days, ranging from 7 days to 18 months. In six out of eight patients the average time between the trauma and features of small bowel obstruction was 50 to 150 days (Table 2).


One patient had portal vein thrombosis with intestinal obstruction one week after the trauma (Figure 4). CT scan of the abdomen showed a fresh occlusive thrombus involving the portal vein, extending into the right branch and proximally into the superior mesenteric vein with luminal narrowing in the distal small boweland proximal dilatation, suggestive of an ischaemic stricture.
Seven patients underwent resection and anastomosis, while in one patient an ileostomy was performed proximal to the obstruction. The mean hospital stay after surgery was seven days, ranging from six to nine days. Wound infection occurred in two patients, and otherwise they had an uneventful recovery. There was no mortality.
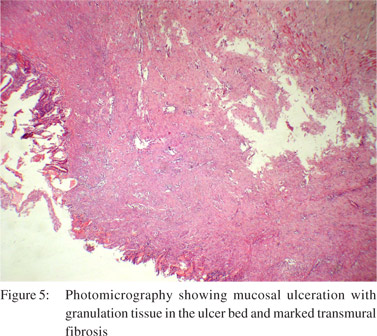
Histopathology (Figure 5) in all cases revealed findings compatible with an ischaemic stricture i.e. mucosal and submucosal ulceration with necrosis and increased vascularity in the submucosa. Diffuse, marked transmural chronic inflammation and fibrosis was observed. The mesentery showed fibrosis, increased vascularity and smooth muscle proliferation.
Discussion
Small bowel stricture following a history of abdominal trauma is a rare cause of small bowel obstruction and there have been few reports examining its occurrence. They have usually followed road traffic accidents, steering wheel and seat belt injuries or direct assaults.[4] In these cases visible signs of injury may not be always present.[5]
The etiology of these strictures is usually ischaemia secondary to mesenteric tears parallel and close to the involved segment, but occasionally direct injury to the bowel wall with subserosal haematoma formation may also result in subsequent stenosis.[6] The proximal jejunum and terminal ileum have been reported as the most common sites involved.[7]
In most cases the patient is managed conservatively till resolution of the initial symptoms of trauma. However, symptoms of small-bowel obstruction appear four to eight weeks5 after the initial trauma; though in some cases it has been reported to occur as early as one week to as long as twenty six years after the injury.[2,3]
The pathological factor causing small bowel stricture is probably local ischaemia due to injury to the mesentery that impairs the blood supply to the bowel, resulting in a stenotic segment adjacent to the mesenteric tear. This heals by fibrosis and the subsequent stricture causes the symptoms that usually have a delayed onset. This mode of injury afflicts the proximal jejunum and distal ileum more commonly, perhaps because the mesentery is fixed at these points, and is more likely to tear in response to a shearing force.[8]
Another possible mechanism for local ischaemia may be the development of hemorrhagic mucosal infarctions caused by direct trauma inflicted on the small bowel. Subsequent healing of these infarctions by fibrosis results in cicatricial stenosis and secondary small bowel obstruction.[6]
Three of our cases underwent laparotomy or laparoscopy during their index episode of trauma hence the possibility of adhesions causing the obstruction was a possibility. However in all three cases there was only a single stricture, without any local anchoring adhesion or band and the single strictures were ischaemic in origin on histopathological examination.
Portal vein thrombosis following blunt trauma to the abdomen is rare. The usual factors implicated for portal vein thrombosis include decrease in portal flow as in cirrhosis, hepatobiliary malignancies and inflammatory processes in the abdomen, or endothelial lesions which initiate thrombus formation due to trauma or surgical injury as after a splenectomy.[9,10] These etiologies were absent in our patient as were any coagulation disorders. In a study by Mattox et al[11] involving 2000 patients who experienced trauma and underwent surgery, only 1% of patients (n=22) had portal vein injury. Seventeen portal vein injuries were secondary to gunshot wounds, 3 to stab wounds and 2 to blunt trauma with only 2 patients overall with blunt abdominal trauma. Pearl et al[12] showed that out of 18,900 patients who sustained injury during a 10 year period only 15 patients sustained portal vein injury which was the result of penetrating abdominal trauma. In fact only nine cases of portal vein thrombosis following trauma have been reported in the literature.[12,13,14,15] In 90% of these cases penetrating trauma was responsible for inciting the thrombotic pathology.[16] The time interval between trauma and thrombosis has ranged from 7 days to 6 months.[17,18] However in our patient none of these causes were found and we attributed the cause of thrombosis to the initial blunt abdominal trauma received by the patient. The patient presented with intestinal obstruction after one week of trauma.
To the best of our knowledge, this is the largest case series on small bowel strictures with a delayed presentation following a prior history of abdominal trauma. Our experience suggests that the possibilityofischaemic stricture should be kept in mind in patients who present with recurrent abdominal pain with or without vomiting and abdominal distension, following a previous episode of blunt abdominal trauma.
References
- Bougard V, Avisse C, Patey M, Germain D, Levy-Chazal N,Delattre JF. Double ischemic ileal stenosis secondary to mesenteric injury after blunt abdominal trauma. World J Gastroenterol. 2008;14:143–5.
- Hirota C, Iida M, Aoyagi K, Matsumoto T, Yao T, Fujishima M. Posttraumatic intestinal stenosis: clinical and radiographic features in four patients. Radiology. 1995;194:813–5.
- Vanderschot PM, Broos PL, Gruwez JA. Stenosis of the small bowel after blunt abdominal trauma. Unfallchirurg. 1992;95:71–3.
- Gray J, Garstin I. Intestinal obstruction following blunt abdominal trauma. Ulster Med J. 2002;71:139–41.
- Lane TM, Williams TG. Small bowel obstruction following blunt abdominal trauma. Injury. 1998;29:484–5.
- Lane TM.Small bowel obstruction after blunt trauma. J R Soc Med. 2000;93:498.
- Marks CG, Nolan DJ, Piris J, Webster CU. Small bowel strictures after blunt abdominal trauma. Br J Surg. 1979;66:663–4.
- Counseller VS, McCormack CJ. Subcutaneous perforation of the jejunum. Ann Surg. 1935;102:365–74.
- Eguchi A, Hashizume M, Kitano S, Tanoue K, Wada H, Sugimachi K. High rate of portal thrombosis after splenectomy in patients with esophageal varices and idiopathic portal hypertension. Arch Surg. 1991;126:752–5.
- Olson MM, Ilada PB, Apelgren KN. Portal veinthrombosis. Surg Endosc. 2003;17:1322.
- Mattox KL, Espada R, Beall AR Jr. Traumatic injury to the portal vein. Ann Surg. 1975;181:519–22.
- Pearl J, Chao A, Kennedy S, Paul B, Rhee P. Traumatic injuries to the portal vein: case study. J Trauma. 2004;56:779–82.
- Duvoux C, Radier C, Gouault-Heilmann M, Texier JP, Le Cudonnec B, Dhumeaux D. A rare cause of portal vein thrombosis: closed abdominal trauma. Gastroenterol Clin Biol. 1994;18:165–7.
- Taylor TV, Torrance B. Portal vein thrombosis following a seatbelt injury. J R Coll Surg Edinb. 1978;23:88–9.
- Maddrey WC, Sen Gupta KP, Mallik KC, Iber FL, Basu AK. Extrahepatic obstruction of the portal venous system. Surg Gynecol Obstet. 1968;127:989–98.
- Feliciano DV. Abdominal vascular injuries. Surg Clin North Am. 1988;68:741–55.
- Gopal SV, Smith I, Malka V. Acute portal venous thrombosis after blunt abdominal trauma. Am J Emerg Med. 2009;27:372.e1–372.e3.
- Gonzalez F, Condat B, Deltenre P, Mathurin P, Paris JC, Dharancy S. Extensive portal vein thrombosis related to abdominal trauma. Gastroenterol Clin Biol. 2006;30:314–6.
|