48uep6bbphidvals|452
48uep6bbph|2000F98CTab_Articles|Fulltext
Anastomotic obstruction with recurrent cholangitis is a well
recognised complication after a bilioenteric anastomosis and
leads to bile stasis with stone formation.[1] The cause is usually
a stricture at the site of the anastomosis and it is also, less
commonly, due to obstruction of the Roux loop by volvulus or
jejunojejunal intussusceptions.[2,3]
We report here an unusual cause of obstruction of the Roux
loop of a hepaticojejunostomy.
Case report
A 57 year old female presented with a one month history of
pain in the right hypochondrium, jaundice and a vague lump
under the right costal margin. Nine years ago she had had an
emergency Roux-en-Y hepaticojejunostomy for a biliary fistula
which had followed a laparoscopic cholecystectomy. However,
eight months after this procedure she began to get recurrent
attacks of cholangitis and investigations revealed a complete
stricture at the anastomotic site. For this a self-expanding
metallic stent was placed percutaneously and transhepatically
across the stricture and she was completely relieved of her
symptoms till she began to experience symptoms of cholangitis
a month ago.
Physical examination of the patient revealed that she had
jaundice with a vague, tender, soft mass in the right
hypochondrium. Liver function tests showed elevated bilirubin
(1.9 mg/dl), alkaline phosphatase (279 IU/l) and gamma glutamyl
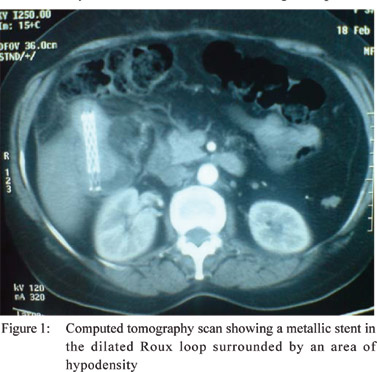
transpeptidase (117 IU /l) levels. Computed tomography of the
abdomen (Figure 1) and magnetic resonance cholangiography
revealed dilatation of the intrahepatic biliary radicles, a patent
hepaticojejunostomy site and a Roux loop which was being
obstructed by a metallic stent which had migrated past the anastomosis. There was an area of hyperdensity around the
stent.
At laparotomy, we found a Roux loop which was obstructed
approximately 15 cm below the anastomosis by a hard
intraluminal mass. We resected a portion of the unhealthy and
nearly perforated jejunal loop containing the mass and
performed an end-to-end jejunojejunostomy. On opening the
resected bowel we discovered that the hard mass consisted of
a stone which had formed around a metallic stent (Figure 2).
Her postoperative period was uneventful and the liver function
tests gradually returned to normal. She was asymptomatic at
one year follow up visit.

Discussion
We described here a case of stent migration causing Roux
loop obstruction and bile stasis nine years following a
hepaticojejunostomy for a biliary fistula and metallic stent
placement for a subsequent anastomotic stricture.
Roux-en-Y hepaticojejunostomy has been associated with
various complications. Common complications include
anastomotic stricture, recurrent calculi and biliary sepsis.
Uncommon complications include calculi or stricture of the
intrahepatic duct, malformed or twisted jejunum loop, too long
or too short proximal jejunum, and adhesion of the intestinal
loop.[4]
Patients who have had a hepaticojejunostomy for
pancreatic and biliary cancers may occasionally develop Roux
loop obstruction due to disease recurrence[5] but stone
formation leading to Roux loop obstruction has been rarely reported,[6,7,8] with enterolith formation around a stent in the Roux
loop seen only after liver transplantation.[9,10]
References
- Rerknimitr R, Sherman S, Fogel EL, Kalayci C, Lumeng L,
Chalasani N, et al. Bilary tract complications after orthotopic
liver transplantation with choledochocholedochostomy:
endoscopic findings and results of therapy. Gastrointest Endosc.
2002;55:224–31.
- Jurim O, Shaked A, Rose S, Busuttil R. Volvulus of the Roux-en-
Y hepaticojejunostomy. A rare complication manifested by
recurrent ascending cholangitis. Int Surg. 1994;79:176–7.
- Shieh CS, Chuang JH , Huang SC. Retrograde intussusception
after Roux-en-Y hepaticojejunostomy for choledochal cyst.
Pediatr Surg Int. 1995;10:398–9.
- Li Z, Cui N, Chen L. Treatment experience of subsequent
complications after Roux-en-Y biliojejunostomy. Eur Surg Res.
2009;43:34–8.
- Holland CL, Olliff SP, Olliff JF. Case report: ultrasound diagnosis
of obstructed Roux loop after cancer of the pancreas or bile duct.
Br J Radiol. 1994;67:309–12.
- Tan WS, Chung AY, Low AS, Cheah FK, Ong SC. Enterolith
formation in the roux limb hepaticojejunostomy. Dig Dis Sci.
2007;52:3214–6.
- Shimamura K, Otani T, Yamazaki T, Kuwabara S, Katayanagi N,
Yamamoto M, et al. Jejunal loop obstruction by a gallstone from
hepaticojejunostomy-induced acute cholangitis: report of a case.
Surg Today. 2006;36:737–40.
- De Moor V, El Nakadi I, Jeanmart J, Gelin M, Donckier V.
Cholangitis caused by Roux-en-Y hepaticojejunostomy
Obstruction by a biliary stone after liver transplantation.
Transplantation. 2003;75:416–8.
- Kawagishi N, Matsuo C, Takeda I, Miyagi S, Satoh K, Akamatsu
Y, et al. Obstructive jaundice caused by biliary stone formation
around the stent after liver transplantation. Pediatr Transplant.
2006;10:835–7.
- Khalaf H, Al-Suhaibani H, Al-Mehaidib A, Shabib S, Bhuiyan
J, Khuroo MS, et al. Roux-En-Y jejunal loop obstruction by a
giant stent-related stone following liver transplantation. Liver
Transpl. 2005;11:1448–9.