48uep6bbphidvals|401
48uep6bbph|2000F98CTab_Articles|Fulltext
Introduction
Polyps are common in the colon. There are different types of polyps which can occur in the colon. Different polyps have different criteria for their diagnosis, depending on the number and site of occurrence in the colon. However, occurrence of multiple true inflammatory polyps mimicking polyposis syndrome has neither been described in the literature nor does it have any criteria to diagnose it.
Case Report
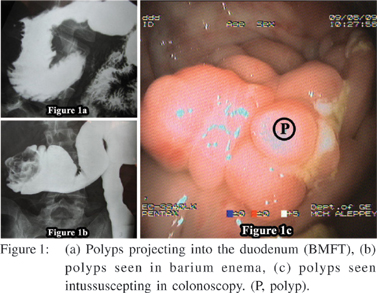
A 38 yr old male patient presented with history of recurrent bilious vomiting and abdominal distention for a period of 3 yrs. At the onset of the disease, patient underwent investigations and was found to have a lesion in the illeocecal area, biopsy of which was inconclusive. Following this, the patient received a trial course of anti-tubercular drugs (RNTCP) for 6 months. However, there was no improvement in symptoms. On examination his vitals were stable. He had lost 17 kg of weight over a period of 3 yrs. He had no cutaneous markers of any disease. Abdomen was soft and did not reveal any mass lesion. Per rectal examination was normal. Routine blood investigations were normal. He underwent a barium examination (Barium meal follow through (BMFT) + barium enema). In the BMFT as the barium was not entering into the colon, a barium enema was also taken. BMFT showed (Figure 1a) a lesion compressing and protruding into the lumen of the duodenum. Barium enema (Figure 1b) showed a lesion in the region of hepatic flexure, with a polypoidal appearance. Colonoscopy(Figure 1c) showed multiple polypoidal lesion at 70 cm from the anal verge. No lumen could be visualized from that point. Biopsy showed only non specific lymphoid infiltrates.
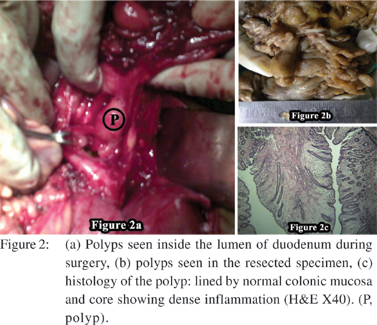
The patient underwent surgery, which revealed a pulled up caecum. There was an inflammatory mass in the region of right upper quadrant. When the colon was opened by a small incision there was a polypoidal mass which was compressing and protruding into the region of duodenum. The lesion had perforated the colon and the surgeons were not able to pull back the lesion from the duodenum. Hence the duodenum was opened, lumen of which showed the polypoidal lesion (Figure 2a). The lesion was pulled back and the rent in the duodenum was repaired. A right hemicolectomy was also done. Gross specimen showed multiple small elongated polyps (Figure 2b) and an area of thinning and perforation in the colon. Histology was suggestive of inflammatory polyps with dense chronic inflammation in the stroma of the polyps (Figure 2c). Patient became asymptomatic following surgery and has put on 15 kgs weight.
Discussion
Inflammatory pseudopolyps are common in patients with inflammatory bowel disease. But there are only a few reports in the literature regarding true inflammatory polyps. Even though there are descriptions about inflammatory polyps mimicking polyposis syndrome,[1] there are no such case reports in the literature. Inflammatory polyps have been reported following ischemic colitis.[2] Any inflammation in the region of illeocecal area can predispose the patient for the development of polyps.It can occur with amebic colitis[3] and schistosomiasis.[4] Even though we have criteria to diagnose familial adenomatous polyposis (FAP), juvenile polyps and hyper plastic polyps, we do not have criteria to diagnose inflammatory polyps. This may be because of dearth of data.
Our case is unique because the patient had multiple true inflammatory polyps mimicking polyposis syndrome. These benign polyps were causing intussusception and coloduodenal fistula.
References
1. Itzkowitz SH, Rochester J. Colonic polyps and polyposis syndrome, In: Feldman M, Friedman LS, Brandt LJ, editors. Sleisenger and Fordtran’s gastrointestinal and liver disease. 8th edn. Saunders; 2006.p.2735.
2. Pidala MJ, Slezak FA, Hlivko TJ. Delayed presentation of an inflammatory polyp following colonic ischemia. Am Surg. 1993;59:315–8.
3. Ciftci AO, Karnak I, Senocak ME, Kale G, Buyukpamukcu N. Spectrum of complicated intestinal amebiasis through resected specimens: incidence and outcome. J Pediatr Surg. 1999;34:1369–73.
4. Yu XR, Chen PH, Xu JY, Xiao S, Shan ZJ, Zhu SJ. Histological classification of schistosomal egg induced polyps of colon and their clinical significance. An analysis of 272 cases. Chin Med J (Engl). 1991;104:64–70.