48uep6bbphidvals|389
48uep6bbph|2000F98CTab_Articles|Fulltext
Introduction
Anatomic variations of the visceral arteries, particularly those concerning celiac trunk and superior mesenteric artery are well known in medical literature.[1,2] Knowledge of these variations is important in the accurate interpretation of disease in diagnostic imaging as well as in deciding the optimum elective procedure in surgical or interventional radiological management.[3] However, there are some more exceptional anatomical variations that may puzzle the surgeons and vascular radiologists dealing with intra abdominal disease. One such case involving the varying branching pattern celiac trunk (CT) and superior mesenteric artery (SMA) is reported here.
Celiac trunk (Figure 1) is the first ventral branch of abdominal aorta arising just below the aortic hiatus at the level of T12-L1. It divides into left gastric artery (LGA), common hepatic artery (CHA) and splenic artery (SA).[4] This trifurcation was first described by Haller in 1756. This “Tripus Halleri” was and is still considered to be the normal appearance of CT.[5]

SMA is the second ventral branch of abdominal aorta arising at the level of L1. Its normal branches include inferior pancreaticoduodenal, jejunal, ileal, ileocolic, right colic and middle colic arteries.[4]
Methods
Anomalous arrangement of the arteries arising from the CT and SMA was found during a cadaveric dissection in the department of Anatomy, PGIMER, Chandigarh. These findings were photographed, schematic diagrams of the arteries were made and length and external diameters of the arteries were measured using a sliding vernier calliper (accuracy 0.02 mm, Mitutoyao, Kawasaki, Kanagawa, Japan).
Results
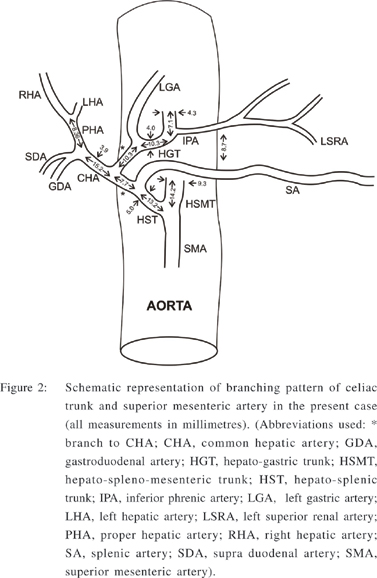
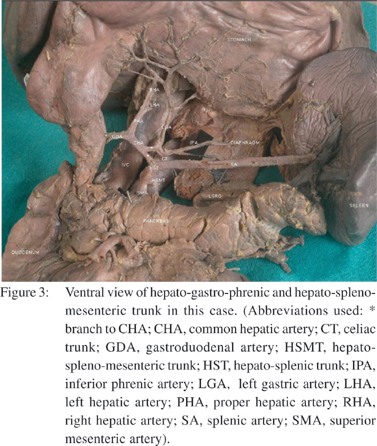
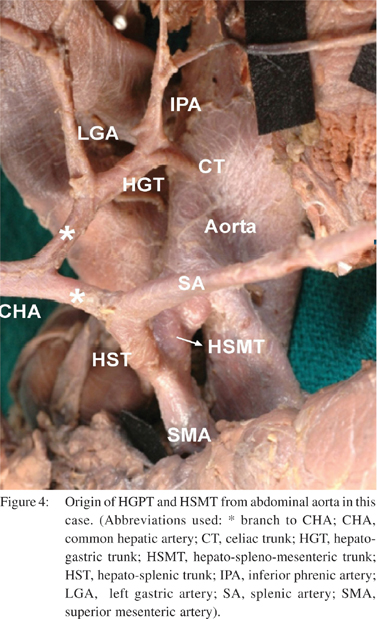
The following variations were observed in the branching pattern of celiac trunk (CT) and superior mesenteric artery (SMA) (Figures 2,3,4):
1. Hepato-gastro-phrenic trunk (HGPT) vis-à-vis celiac trunk (CT) Celiac trunk of the length of 7.1 mm and external diameter of 4.3 mm arose from the ventral aspect of abdominal aorta. It gave left inferior phrenic artery (IPA) as its first branch and continued as hepato-gastric trunk (HGT). Left IPA, during its course towards diaphragm gave a branch to left suprarenal gland. HGT (external diameter 4.0 mm) after a length of 10.3 mm divided into left gastric artery (LGA) and a branch to common hepatic artery (CHA). Splenic artery (SA) did not arise from CT.
2. Hepato-spleno-mesenteric trunk (HSMT) vis-à-vis superior mesenteric artery (SMA): SMA arose about 8.7 mm below the origin of CT, from the ventral aspect of abdominal aorta. SMA (external diameter 9.3 mm) after a length of 14.2 mm gave hepato-splenic trunk (HST) as its first branch and then continued in its normal course. Hepato-splenic trunk (HST) divided into splenic artery and a branch to common hepatic artery.
3. Common hepatic artery (CHA) was thus formed by the union of a branch arising from HGT and another branch arising from HST.
4. Thus, in this case, CT and SMA may be named as Hepatogastro- phrenic trunk (HGPT) and Hepato-splenomesenteric trunk (HSMT) respectively.
5. Inferior mesenteric artery showed no anomalous feature.
Discussion
Understanding of the CT and SMA anatomy as well as knowledge of type of anatomical variants involving these vessels is essential for a proper pre-operative vascular planning in surgical or radiological procedures in the upper abdomen.
Embryology of celiac trunk and superior mesenteric artery
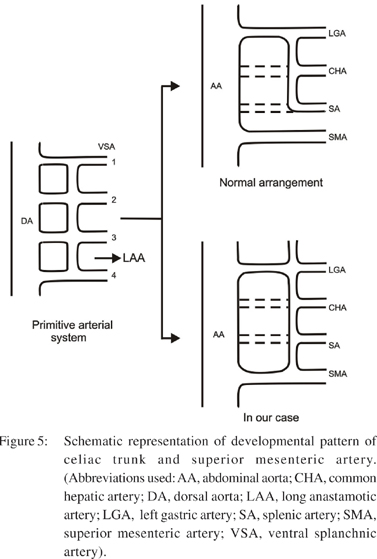
Tandler provided an embryological explanation for the variations of CT and SMA in 1904.6 During development, three group of collateral anastamotic arteries, arise from the abdominal aorta as dorsal, lateral and ventral branches. The latter develop initially as paired vessels, which then coalesce in the median line to form the four roots for the gut, the four roots being connected by ventral longitudinal anastomosis. In the majority of cases, first three roots coalesce to form CT and separate from the fourth root. The future SMA is developed from the fourth root, which migrates caudally with the ventral migration of gut. The variations in these arteries arise from differences in the pattern of the partial disappear rance or the survival of the ventral splanchnic arteries and the ventral longitudinal channel (Figure 5).7 Adachi (1928) examined the CT of 252 subjects and classified the pattern of ramification of the CT into six types and showed diversity within each pattern.[8]
Since then, there have been many reports on the arterial patternsof the CT based on Adachi’s classification.[9,10] In the present study, LGA was seen to be arising from CT, SA arose from SMA and CHA was receiving contributions from both CT and SMA. This type of branching pattern of CT and SMA is a rare variation that couldn’t be described by the Adachi’s classification.
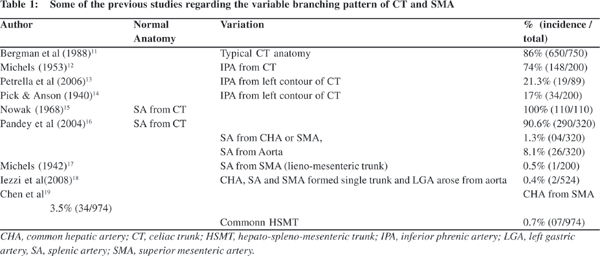
Some of the previous studies regarding the variable branching pattern of CT and SMA that have been described in the literature are given in Table 1.
Clinical implication
While vascular anomalies are usually asymptomatic they may become important in patients undergoing surgical, oncologic or interventional procedures like lymphadenectomy around hepato-spleno-mesenteric trunk, celiac artery compression syndrome, aortic replacement with re-implantation of the trunk or chemoembolisation of liver malignancies, can be potentially life threatening because of large visceral territory supplied by a single vessel.[20]
We re-emphasize the importance of thorough knowledge of normal anatomy and its variations in clinical medicine. Many of the complications could be avoided with the accurate knowledge of the anatomic variations. We believe that, this case will take its place in the literature and play a significant role in the surgical intervention in the abdominal region and also in angiographies.
References
1. Lippert H, Pabst R. Arterial variations in man. München, JF Bergmann, 1985.pp.71–3.
2. VanDamme JP, Bonte J. Vascular anatomy in abdominal surgery. Georg Thieme Verlag, Stuttgart; 1990.pp.4–42.
3. Oran I, Yesildag A, Memis A. Aortic origin of right hepatic artery and superior mesenteric origin of splenic artery: two rare variations demonstrated angiographically. Surg Radiol Anat. 2001;23:349–52.
4. Standring S, Borley NR, Collins P, Crossman AR, Gatzoulis MA, Healy JC, et al., editors. Gray’s anatomy. The anatomical basis of clinical practice. 40th edn. New York: Churchill Livingstone; 2008.
5. Vandamme JP, Bonte J. The branches of the celiac trunk. Acta Anat (Basel). 1985;122:110–4.
6. Tandler J. Uber die varietaten der arteria coeliaca und deren entwicklung. Anat Hefte. 1904;25:472–500.
7. Osawa T, Feng XY, Sasaki N, Nagato S, Matsumoto Y, Onodera M, et al. Rare case of the inferior mesenteric artery and the common hepatic artery arising from the superior mesenteric artery. Clin Anat. 2004;17:518–21.
8. Adachi B. Das arterien aystem der japaner, Band II. Kyoto: Verlag der Keiserlich-Japanischen Universitat zu Kyoto, Maruzen Publishing Co; 1928.pp.28,38,54.
9. Morita M. Reports and conception of three anomalous cases of the celiac and superior mesenteric arteries. Igaku Kenkyu. 1935;9:1993–2006 (in Japanese).
10. Saga T, Hirao T, Kitashima S, Watanabe K, Nohno M, Araki Y, et al. An anomalous case of the left gastric artery, the splenic artery and hepato-mesenteric trunk independently arising from the abdominal aorta. Kurume Med J. 2005;52:49–52.
11. Bergman RA, Thompson SA, Afifi AK, Saadeh FA. Compendium of human anatomic variation. Baltimore: Urban and Schwarzenberg; 1988.p.77–80,83.
12. Michels NA. Variational anatomy of the hepatic, cystic, and retroduodenal arteries; a statistical analysis of their origin, distribution, and relations to the biliary ducts in two hundred bodies. AMA Arch Surg. 1953;66:20–34.
13. Petrella S, Rodriguez C, Sgrott EA, Fernandes G, Marques SR, Prates JC. Origin of inferior phrenic arteries in the celiac trunk. Int J Morphol. 2006;24:275–8.
14. Pick JW, Anson BJ. Inferior phrenic artery: Origin and suprarenal branches. Anat Rec. 1940;78:413–27.
15. Nowak M. Variation of the celiac trunk in man. Folia Morphol. 1968;27:51–69.
16. Pandey SK, Bhattacharya S, Mishra RN, Shukla VK. Anatomical variations of the splenic artery and its clinical implications. Clin Anat. 2004;17:497–502.
17. Michels NA. The variational anatomy of the spleen and splenicartery. Am J Anat. 1942;70:21–72.
18. Iezzi R, Cotroneo AR, Giancristofaro D, Santoro M, Storto ML. Multidetector-row CT angiographic imaging of the celiac trunk: anatomy and normal variants. Surg Radiol Anat. 2008;30:303–10.
19. Chen H, Yano R, Emura S, Shoumura S. Anatomic variation of the celiac trunk with special reference to hepatic artery patterns. Ann Anat. 2009;191:399–407.
20. Losanoff JE, Millis JM, Harland RC, Testa G. Hepato-splenomesenteric trunk. J Am Coll Surg. 2007;204:511.