|
Ashok Teja, Aswini K Pujahari Department of Surgery, Great Eastern Medical School and Hospital, Ragolu, Srikakulum, AP, India.
Corresponding Author:
Dr Aswini K Pujahari Email: akpujahar@gmail.com
48uep6bbphidcol2|ID 48uep6bbphidvals|2974 48uep6bbph|2000F98CTab_Articles|Fulltext Ingestion of a foreign body is not uncommon. Once it passes the pharynx, it usually comes out of the anus, unless it is a long, sharp, or a chemical-laden FB, when perforation/penetration is a possibility.1 However, FB in the common bile duct (CBD) is uncommon, and FB piercing common Bile duct (CBD) is very unusual and uncommon. The common foreign bodies in the CBD are usually left by surgeons or therapeutic endoscopist. They are non-absorbable sutures2 or leftover parts of a tube or stent.3,4 Rarely ingested long and sharp FB penetrate CBD accidentally. Reported cases include a toothpick and a Ligaclip post lap cholecystectomy.5-7 Very rarely during blast shrapnel and metal fragments are seen after a blast injury,8,9 but vegetable and digestible FB causing CBD stone causing cholangitis is being reported for the first time.
Case Report
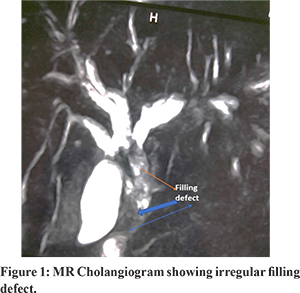
A fifty-seven-year-old male manual labourer had presented to the outpatient department with a history of fever and passage of yellow urine of a one-week duration. He had a history of fever of 101-103° F with chills with maximum temperature in the evening hours. He was having itching at night and passing pale stool. He gave a history of upper abdominal pain, and vomiting six months back lasted for three days. His wife attributed this pain and vomiting to alcohol intake, and he improved without any hospitalization. He had no co-morbidity. While being treated for the present complaint, a local physician noted raised bilirubin and creatinine for which referred for hospitalization. On examination, he was jaundiced, with a fever of 100.4°F, pulse rate 100/min, and normal BP. The liver was 4cm below the costal margin at the midclavicular line, tender, smooth, and firm. The gall bladder was not palpable. There were no other abdominal findings. He was given intravenous antibiotics (Cefaperazone1000 mg + Sulbactam 500 mg twice daily and Metronidazole 500 mg every 8hourly) besides plenty of oral fluids and Vit K 10 mg IM daily. MRCP showed dilated CBD with a filling defect (Figure 1). He improved in three days. Endoscopic CBD stone clearance was unsuccessful except for some sludge, and thus, the patient was taken up for open surgery.
Intraoperatively, the pylorus and the first part of the duodenum were covered with omentum. The CBD was dilated, and the gall bladder did not have stones. Omentum was lysed, and cholecystectomy was done. The thick-walled CBD was approached via the cystic duct lumen for confirmation (Figure 2). It was opened at 12 o clock position just superior to the duodenum. After clearing the CBD, choledocho-duodenostomy was done using PDS sutures, fearing the ulcerated lower CBD’s possible stricture. After analysing the CBD stone, the two sticks, like substances and stone, were found (Figure 3). On showing this to his wife, it was found out to be a Curry leaf stem, which became evident after drying and separation of stone. The patient recovered well. The liver and renal parameters normalized in three weeks. He remained asymptomatic for 3 years follow up.
Discussion
Usual CBD foreign bodies are left by surgeons and endoscopists. These include non-absorbable sutures, gauze, and forgotten stent.10 They act as a nidus for stone formation, and thus, the stone load is often directly proportional to the duration of retention.11,12 Other foreign bodies can enter the CBD via three routes: (a) by piercing the duodenal wall (first part) because of their intimate relation, as in toothpick entry (b) following bilio-enteric anastomosis following a pancreaticoduodenectomy, a fishbone or (c) through ampulla. The authors justified the later, highly un-probable hypothesis for a long pin.5,13,14 The curry leaf (Murraya koenigii) is a tropical tree in the family Rutaceae. It is used as a spice in India. 12 to 15 leaf are usually present on one stem (Figure 3). There is literature on the use and benefit of curry leaf. Anti-pseudomonal activity was demonstrated from its extract.15 The staple meal in south Indian states of rice, rasam (watery tamarind preparation) and shamber (dal preparation with vegetables), has a short gastric time and might not have enough time to soften the stem. During gastric peristalsis, the stomach wall may have pushed the stem, which penetrated the duodenal wall and CBD. Once inside the CBD, the stone formation would have come with time. The MRCP showing an unusual filling defect (Figure 1) and deformity of the first part duodenum at surgery is a corroborating factor (Figure 2). Such a FB is usually detected while chewing the food when the chewing is slow. Such events are reported to be common in people who chew and swallow their food quickly. We found no literature on any vegetable food product penetrating CBD so far, which is going to be the first such kind in the medical literature.
Conclusion
Foreign body ingestion is a common occurrence. Nevertheless, penetration to CBD is very rare. Curry leaf stem penetrating the CBD, forming nidus for stone, and causing cholangitis is reported for the first time.
References - Peter Ambe, Sebastian A Weber, Mathias Schauer, and Wolfram T Knoefel, Review article. Swallowed Foreign Bodies in Adults. DtschArztebl Int. 2012.
- Qiang L, Liang T, Xingyu W at. el Bile duct stone formation around a proline suture after cholangioenterostomy. Pak J Med Sci. 2016.
- Barai V, Hedawoo J, Changole S. Forgotten CBD stent (102 months) with stone-stent complex: A case report Int J Surg Case Rep. 2017.
- Upwanshi MH, Shaikh ST, Ghetla SR, Shetty TS. De novo Choledocholithiasis in Retained Common Bile Duct Stent. J Clin Diagn Res. 2015.
- V. O. Brunaldi, M. O. Brunaldi, R. Masagao et,al . Toothpick inside the Common Bile Duct: A Case Report and Literature Review Case Rep Med. 2017.
- Krishn Kant Rawal Migration of Surgical Clips into the Common Bile Duct after Laparoscopic Cholecystectomy Case Rep Gastroenterol. 2017;10: 787–792.
- Jun-wen Qu, Gui-yang Wang, Zhi-qing Yuan, and Ke-wei Li. Case report-Hem-o-lok Clips Migration: An Easily Neglected Complication after Laparoscopic Biliary Surgery Case Reports in Surgery. 2017
- Somi MH, Rezaeifar P. Shrapnel splinter in the common bile duct. Arch Iran Med. 2010; 13:53-6.
- Gottschalk U, Weber B, Felfe R. Obstructive jaundice after grenade splinter injury 49 years ago. Z Gastroenterol. 1993 ;31:201-4.
- Andrews S. Gallstone size related to incidence of post cholecystectomy retained common bile duct stones. Int J Surg. 2013; 11:319–321.
- Sohn SH, Park JH, Kim KH, Kim TN. Complications and management of forgotten long-term biliary stents World J Gastroenterol. 2017;23:622-628.
- Cimsit B, Keskin M, Ozden I, Alper A. Obstructive jaundice due to a textiloma mimicking a common bile duct stone. J Hepatobiliary Pancreat Surg. 2006;13:172-3.
- Sakakida T. • Sato H. • Doi T. at. el•. A Bile Duct Stone Formation around a fish bone as a nidus after Pancreatoduodenectomy: Single Case. Case Reports in Gastroenterology. Case Rep Gastroenterol 2018;12:69–75
- Ranjan Dias and ParackramaDharmaratne Ingested foreign body in the common bile duct.J Indian Assoc Pediatr Surg. 2012; 17: 31–32.
- Sankar Ganesh, Ravishankar Rai; et al. (2015). “In vitro antibiofilm activity of Murraya koenigii essential oil extracted using supercritical fluid CO2 method against Pseudomonas aeruginosa PAO1”. Natural Product Research. 29: 2295–2298.
|