|
Ajay K Jain1, Sudesh Sharda2, Amit D Joshi1, Suchita Jain3 Department of 1Gastroenterology, 2General and Minimal Access Surgey, Department of 3Radiodiagnosis and Imaging, Chothram Hospital & Research Centre, Indore, Madhya Pradesh, India.
Corresponding Author:
Dr Ajay K. Jain Email: ajayvjain@yahoo.com
48uep6bbphidcol2|ID 48uep6bbphidvals|2970 48uep6bbph|2000F98CTab_Articles|Fulltext Penetrating rectal injuries in civilian surgical practice are mostly due to gun-shot injuries or stab injuries in buttock area1. Treatment algorithm of these penetrating injuries depends upon whether its a gun-shot or stab wound. Irrespective, the management of these injuries is challenging and depends upon associated internal injuries. Fundamental management principles of rectal injury secondary to stab wound include direct primary closure, fecal diversion, presacral drainage or distal rectal washout.2 We report a case of stab injury to the natal cleft region with the rectal injury which was successfully managed endoscopically by using over-the-scope-clip (OTSC).
Case Report
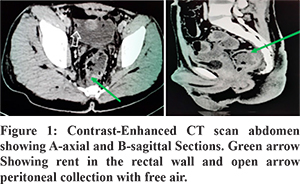
A twenty-year-old male with a history of stab injury to the natal cleft region presented with symptoms of lower abdominal pain. He was hemodynamically stable. There was tenderness in both lower quadrants, and pus discharge from the natal cleft wound. He was kept nil by mouth, and given intravenous fluids and antibiotics. The site of injury in the natal cleft area was locally explored, and a drain was placed for pus drainage. Contrast-enhanced CT of the abdomen revealed pneumo-peritoneum, a defect in the right postero-lateral wall of intra-peritoneal part of the rectum, and contrast leak. This defect was about 4-5 mm in diameter and was at about 10 cm from the anal verge (Figure 1). Conservative management was continued because of the small rectal defect. Despite four days of conservative management, the patient continued to have pus discharge from the external wound as well as per rectally. At this stage, flexible sigmoidoscopy revealed a rectal defect at about 10 cm from the anal verge with significant seeping of pus (Figure 2A). As there was no associated internal injury, we decided to close the defect endoscopically using the Over-The-Scope-Clip (OTSC®, Ovesco Endoscopy GmbH, Tübingen, Germany).
We chose OTSC-t with a cap-size of 10.5-12 mm and a depth of six mm. The OTSC-’t’ has teeth with small spikes provides an anchoring effect in the closure of perforation, and a six mm cap depth for better tissue approximation (Figure 2B). Post clip application over the next few days pus discharged stopped entirely with the healing of the external wound. He remained afebrile and was started on regular meals from day three. Follow-up ultrasonography on day five revealed no pneumo-peritoneum or intraperitoneal collection. On follow up at three months, the patient is asymptomatic.
Discussion
Management of stab wounds of the gluteal region is challenging. These wounds may appear trivial; however, in about one-quarter of patients, are associated with injuries to major vessels, nerves, ligaments, and intestine. A study on stab wounds to the buttock revealed that visceral and vascular injuries occur in 10.5% of patients admitted to a large trauma center.3 The most commonly damaged structures following penetrating injury to the buttock are the superior gluteal artery, rectum, small bowel, and colon (each = 5%). Injury to the iliac artery or vein is diagnosed in 3% of patients, while sciatic or lumbosacral nerves injury is rare(1%). If the damage to the rectum is non-destructive, less than 50% of the circumference of the intraperitoneal rectum, it can undergo primary repair. Selective non-operative management of penetrating injuries of the gluteal region in stable patients without significant organ injury is also a successful approach.4 OTSC is a safe and effective therapy for closure of GI defects when it used for primary or rescue therapy5. OTSC clips are now being used successfully for the closure of a variety of acute and chronic defects in the upper and lower gastrointestinal tract. The type of defect is the best predictor of successful long-term closure. There are many advantages of the OTSC clip, which is made up of Nitinol. First, it allows microperfusion of the clipped tissue; therefore, no necrosis of tissue occurs. Second, it adopts continuously to the thickness of the tissue even when the volume of the tissue shrinks over the healing course, thus maintaining consistent compression. Third, it enables dynamic closure rather than static to avoid potentially inadequate closure over time as it can happen in fixed suture loops. The overall success rate of these clips in various defects is about 79%.6 We believe this is the first case of penetrating rectal injury treated successfully by OTSC. In conclusion, penetrating injuries of the rectum without involvement of other associated vascular, bony, or nervous structures can be successfully treated with newer endoscopic accessories like OTSC clips, thereby saving patients from major surgery with associated morbidity.
References - Makrin V, Sorene ED, Soffer D, Weinbroum A, Oron D, Kluger Y. Stab wounds to the gluteal region: A management strategy. J Trauma. 2001;50:707–10
- Ahern DP, Kelly ME, Courtney D, Rausa E, Winter DC. The management of penetrating rectal and anal trauma: A systematic review. Injury. 2017;48:1133–1138.
- Susmallian S, Ezri T, Elis M, Dayan K, Charuzi I, Muggia-Sullam M. Gluteal stab wound is a frequent and potentially dangerous injury. Injury. 2005;36:148-150.
- Velmahos GC, Demetriades D, Toutouzas KG, et al. Selective non-operative management in 1,856 patients with abdominal gun-shot wounds: should routine laparotomy still be the standard of care?. Ann Surg. 2001;234:395-403.
- Haito-Chavez Y, Law JK, Kratt T, et al. International multicenter experience with an over-the-scope clipping device for endoscopic management of GI defects. Gastrointest Endosc. 2014;80:610–622.
- Donatelli G, Cereatti F, Dhumane P, et al. closure of gastrointestinal defects with Ovesco clip: long-term results and clinical implications. Therap Adv Gastroenterol. 2016;9:713-721.
|