Saphalta Baghmar1, Rommel Sandhyav2, Asit Arora2, Ankur Arora31Department of Medical Oncology, 2Department of Hepatopancreatobiliary surgery, ILBS, Vasant Kunj, New Delhi 110070, India 3Consultant Radiologist, Worthing Hospital, Western Sussex NHS Trust
Corresponding Author:
Dr Asit Arora Email: drasitarora@yahoo.com
48uep6bbphidcol2|ID 48uep6bbphidvals|1882 48uep6bbph|2000F98CTab_Articles|Fulltext Carcinoma Gall Bladder (CaGB) is the most common biliary tract malignancy with geographic and ethnic disparities. It is one of the most common malignancies in north India, particularly in females. It has a vague presentation and mostly is detected in advanced stage. We here in report an interesting case which initially presented as liver abscess and latter diagnosed as gall bladder cancer with cardiac metastasis.
Case Report
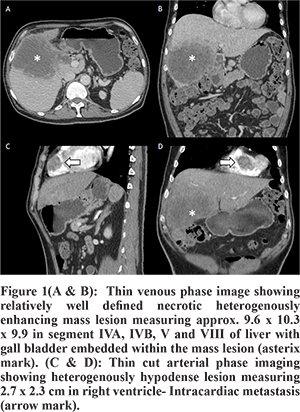
A 55 year old gentleman presented to us with persistent fever and pain abdomen for the last one and half months. He was evaluated elsewhere with USG and CECT of the abdomen. A diagnosis of liver abscess was made and he was treated with antibiotics and percutaneous catheter drainage of the abscess cavity. The catheter was removed after three days. He continued to be symptomatic and was given a long course of antibiotics. At presentation to our hospital he was febrile, septic but hemodynamically stable, anicteric with no lymphadenopathy. Abdominal examination was unremarkable. Blood investigations revealed a raised total count of 21900 c/mm3, normal bilirubin and liver enzymes with raised Serum Alkaline Phosphatase. He was reassessed with CECT which showed a large partly exophytic relatively well defined necrotic heterogenously enhancing mass lesion measuring approx. 9.6 x 10.3 x 9.9 in segment IVA, IVB, V and VIII of liver with gall bladder embedded within the mass lesion (Figure 1A and 1B), with heterogenously hypodense lesion measuring 2.7 x 2.3 cm in right ventricle (Figure 1C and 1D), suggestive of gall bladder cancer with intracardiac metastasis. Tumour markers were evaluated which showed CEA-23.19, CA 19-9 100.5. ECHO showed a 2.5 x 4.6 mm homogenous mass in the Right ventricular apex with no free mobility. FNAC from the gall bladder mass confirmed the diagnosis of gall bladder cancer. In view of his poor performance status he was planned for best supportive care. He succumbed to his disease within 2 months of presentation.
Discussion
Metastatic spread from primary CaGB is usually to the liver and the paraaortic lymph nodes. The modes of dissemination in gallbladder carcinoma are direct, lymphatic, vascular, neural, intraperitoneal, and intraductal. There have been reports of CaGB metastasising to unusual sites like bone1, brain1, ovary 2, spine3, cheek4 and breast5. A handful cases with cardiac metastasis have also been reported.6-9 Gall bladder cancer can very rarely mimic a liver abscess, which may come to light only after drainage or at the time of surgery. We herein report an extremely uncommon combination of two rare presentations of gall bladder cancer in a patient i.e. gall bladder cancer presenting as liver abscess and subsequently developing cardiac metastasis. Cardiac metastasis may develop via lymphatic, haematogenous or direct spread. But myocardial involvement like in our case is usually through haematogenous spread. Most cardiac metastasis are asymptomatic and are detected incidentally or at the time of autopsy.7-10 Autopsy studies of metastatic neoplasms of the heart have reported gallbladder carcinoma as a rare primary site.10 Only one case has been reported of a gall bladder cancer presenting with pyrexia of unknown origin and misdiagnosed as liver abscess on CT, as in our case and later found to have carcinoma only at surgery.11
Conclusion
The case illustrates an unusual presentation of gallbladder carcinoma with a combination of a rare demonstration of it as liver abscess with cardiac metastasis. At the same time, it highlights the highly aggressive nature of gallbladder carcinoma, progressing from asymptomatic to death within two months. Thus an early diagnosis is essential in cases of CaGB and improved imaging modalities and its interpretation supplemented with accurate diag¬nostic markers will potentially help outcomes.
References - Aung Z. Win, Carina M. Aparici, Rare case of gallbladder cancer presenting with metastasis to bone and brain in an African American male discovered by F18-FDG PET/CT, J Biomed Graph Comput. 2013;3(2) 24-29
- Kumar Y, Chahal A, Garg M, Bhutani A. Occult gallbladder carcinoma presenting as a primary ovarian tumor in two women: two case reports and a review of the literature. J Med Case Reports. 2010 Jun 30;4(1):202.
- Joshi MK, Joshi R, Chadha M, Alam SE, Varshneya H, Kumar S. Gall bladder carcinoma presenting with spinal metastasis: a rare phenomenon. Indian J Palliat Care. 2013 May;19(2):113–5.
- Marin H, Bouras AF, Patenôtre P, Boleslawski E, Zerbib P, Pruvot FR, et al. Cheek metastasis from gallbladder adenocarcinoma. J Visc Surg. 2013 Jun;150(3):225–6.
- Shukla P, Roy S, Tiwari V, Mohanti BK. Unusual presentation of metastatic gall bladder cancer. J Cancer Res Ther. 2014 Jun;10(2):397–8.
- Gunjiganvi M, Singh KK, Harsha HS, Bipin T. Cardiac metastasis from gallbladder carcinoma. Int J Surg Case Rep. 2013 Oct 22;4(12):1156–8.
- Suganuma M, Marugami Y, Sakurai Y, Ochiai M, Hasegawa S, Imazu H, et al. Cardiac metastasis from squamous cell carcinoma of gallbladder. J Gastroenterol. 1997 Dec;32(6):852–6.
- Sugezawa A, Hiraoka H, Iizuka Y, Nishimura K, Kishi H, Furuse T, et al. [Heart metastasis of gallbladder cancer--a case report]. Gan No Rinsho Jpn J Cancer Clin. 1987 Apr;33(4):406–10.
- Inoue T, Shiraki K, Fuke H, Yamanaka Y, Miyashita K, Ito K, et al. Cardiac metastases of gallbladder carcinoma. World J Gastroenterol. 2005 Apr 7;11(13):2048–9.
- Hanfling SM. Metastatic cancer to the heart. Review of the literature and report of 127 cases. Circulation. 1960 Sep;22:474–83.
- Singla SL, Garg P, Tahlan RN. Gall bladder carcinoma presenting as liver abscess. Indian J Gastroenterol Off J Indian Soc Gastroenterol. 1998 Apr;17(2):68.
|