48uep6bbphidcol2|ID
48uep6bbphidvals|1878
48uep6bbph|2000F98CTab_Articles|Fulltext
Abnormal rotation and recanalization during embryologic development can lead to variation in pancreatico-biliary ductal anatomy. Usually, the bile duct and pancreatic duct join together at the level of duodenum to form papilla of Vater. During embryogenesis, complete non-union of distal bile duct and ventral pancreatic duct give rise to separate orifice of these two ducts as double papilla. It is a very rare condition and only few cases have been reported in literature.1-4
Case Report
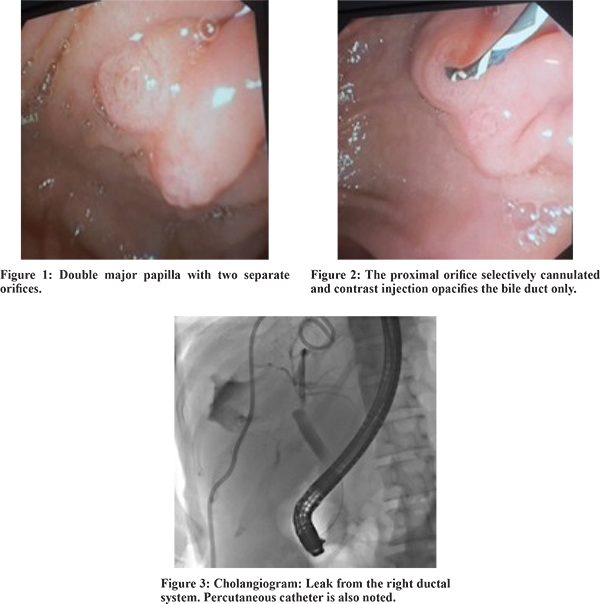
A 60 years female presented with right upper abdominal pain 9 months back and on evaluation was found to have a large hydatid cyst. She underwent exploratory laparotomy and enucleation of the hydatid cyst in another hospital. Post operatively, patient developed bilioma which was drained by percutaneous catheter drainage (PCD). Patient presented to us with persistent drainage of bile through the PCD. On evaluation hemogram and biochemical parameters were as follows: hemoglobin-12.2g/dl, total leucocyte count (TLC) - 9900/mm3, platelet count-173x103/mm3, bilirubin-0.7mg/dl, AST-21 U/L, ALT-15 U/L, APL-182 U/L. Her renal function and coagulogram were normal. In view of persistent bile leak, the patient was taken up for endoscopic retrograde cholangiopancreatography (ERCP), and during the procedure two separate papillary openings were identified (Figure 1). The cranial orifice was located at 11 o’clock position and the caudal orifice was at 7 o’clock position. Selective cannulation of the cranial orifice (biliary orifice) was done (Figure 2) and contrast injected. Following that, only common bile duct was opacified and no opacification of the main pancreatic duct was observed. Cholangiogram revealed leakage of the contrast from the right ductal system (Figure 3). A 7 Fr 7 cm double pigtailstent was placed in the biliary system and following that patient had marked improvement in her symptoms with reduction in the drain output.
Discussion
The apertures of pancreatic and bile ducts opening into the duodenum is called the ampulla of Vater. It is developed early in the 7th week of gestation by fusion of the biliary and pancreatic ducts in closed cavities of the duodenum.5 Fusion of the biliary and pancreatic duct can give rise to 3 different patterns of pancreatico-biliary ductal opening: a common duct where both the duct open into a single opening, separation of the two ductal opening by a partition and complete separation of the two ductal opening giving rise to so called double papilla.6 Double papilla is a very rare condition with one series reporting its incidence to be 0.18% of patients undergoing ERCP.4 In double papilla, the proximal opening drains the bile duct whereas the distal opening drains the pancreatic duct. The bile duct orifice is always located at the upper left of the pancreatic duct orifice.6 This entity usually does not predispose to any disease except for the occasional report of increased risk of bile duct stone due to stasis.7 It also require a differential diagnosis from secondary choledochoduodenal fistula. It is important that the endoscopists are aware of this rare variation so as to prevent unnecessary manipulation of the pancreatic duct and consequent increased risk of post-ERCP pancreatitis. Also, correct identification of the bile duct orifice will virtually exclude the risk of post - ERCP pancreatitis as the pancreatic duct manipulation is avoided because of a separate duct opening.
References
- Katsarelias D, Faisal M, Glavas R, Bartholomä WC. Double papilla of Vater: arare anatomic variant. Endoscopy. 2016;48 Suppl1:E133-4.
- Rana SS, Bhasin DK. Papilla with separate bile and pancreatic duct orifices. JOP2013;10;14:302-3.
- Rajnakova A, Tan WT, Goh PM. Double papilla of Vater: a rare anatomic anomaly observed in endoscopic retrograde cholangiopancreatography. SurgLaparoscEndosc. 1998; 8:345-8.
- Simon MA, Moreira VF, Merono E, Seara JF, del Olmo L. The double papilla of Vater. GastrointestEndosc. 1985;31:353–354
- Ando H. Embryology of the Biliary Tract. Dig Surg2010;27:87–89
- Horiguchi S,Kamisawa T. Major Duodenal Papilla and Its Normal Anatomy. Dig Surg2010;27:90–93
- Kubota K, Fujisawa T, Abe Y, Inamori M, Kirikoshi H, Saito S, et al. Clinical significance of the duodenal papilla in patients with separate orifices for the bile and pancreatic ducts. J Gastroenterol. 2007;42:70-8