48uep6bbphidcol2|ID
48uep6bbphidvals|1802
48uep6bbph|2000F98CTab_Articles|Fulltext
Omental torsion is a rare cause of acute abdomen. Here, we report a rare case of omental torsion, leading to infarction associated with left inguinal hernia. Surgical excision of the infarcted omentum was done and the patient recovered well.
Case Report
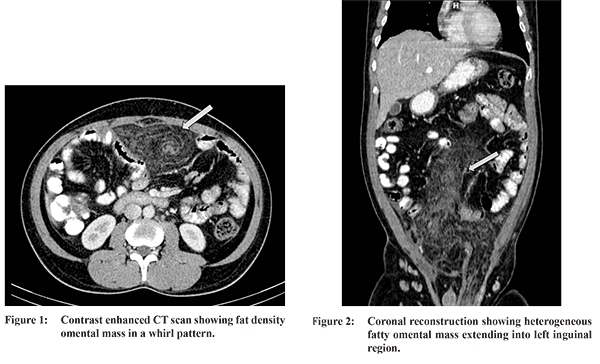
A 38-year-old man presented with a history of abdominal pain since 3 days and inguino-scrotal swelling since 6 months. Physical examination reveal diffuse abdominal tenderness and irreducible left inguinal hernia. Bowel sounds were normal. Laboratory parameters were normal. Plain radiograph of the abdomen was unremarkable. Ultrasound examination demonstrated hyperechoic non-compressible omental mass herniating into left inguinal region. Free fluid was noticed within peritoneal cavity. Plain and contrast CT examination of the abdomen and pelvis revealed a fatty mass consistent with greater omentum. A centre hyperdense structure with surrounding whirling streaks seen suggestive of torsion of vascular pedicle (Figure 1). There was marked stranding of the omentum, continued inferiorly into the inguinal hernia (Figure 2). Surrounding bowel loops were displaced towards periphery by the omental lesion with no evidence of bowel obstruction. Moderate ascites was noted. The patient subsequently underwent exploratory laparotomy, which revealed diffuse infarction of the greater omentum along with omental torsion in the hernial sac (Figure 3). An omentectomy with repair of the left inguinal hernia was performed. Post-operative recovery was uneventful. On histopathology, a diagnosis of omental infarction was confirmed.

Discussion
Twisting of omentum along its long axis results in impaired blood supply and eventually progress to infarction. Ultrasound or CT scan is mandatory as a preoperative diagnostic tool. Surgical excision is the preferred modality of treatment.
1 The majority of cases have right sided torsion and the left sided torsion is rare. As a result of right sided torsion, the presentation usually mimics acute cholecystitis, acute appendicitis, cecal diverticulitis and epiploic appendagitis. The greater susceptibility of the right sided omental torsion is due to its greater length, size, more mobility and less vascularization with poor collateralization.
2 Torsion of the greater omentum can be primary or secondary. Primary (idiopathic) version is much less common and predisposing factors such as bifid omentum, redundant omental veins are suggested in etiology. Secondary torsion is more common, occurring in association with intra- abdominal pre-existing conditions, the internal or external hernia, tumor adhesions and inflammation.
3 On CT scan, the mass is well circumscribed and is composed of fat with internal hyperattenuating streaks which are typically arranged in concentric or spiral pattern. The key to the diagnosis is the presence of concentric linear strands consistent with the torsioned vascular pedicle which are characteristic.
4 This important radiological sign is not present in other omental disease. The whirling pattern may not be apparent is cases where axis of rotation is not prependicular to the transverse scanning plane. Radiological differential diagnosis is lipoma, liposarcoma, angiomyolipoma, teratoma, mesentric lipodystrophy, abdominal panniculitis and fat necrosis secondary to pancreatitis.
References
- Silva E, Carvalho AF, Rocha D, etal. Omental whirl associated with bilateral inguinal hernia: a case report. J Med Case Rep. 2014;8:239.
- Hirano Y, Oyama K, Nozawa H, etal. Left sided omental torsion with inguinal hernia. World J Gastroenterol. 2006;28;12(4):662-664.
- Gupta R., Mittal P., Mittal G. left sided omental torsion with left inguinal hernia : A rare entity. Indian J Gastroenterol. 2011;30(6):287.
- Naffaa LN, Shabb NS, Haddad MC. CT finding of omental torsion and infarction: Case report and review of literature. Clin Imaging. 2003;27(2):116-118.