Upender Shava, Ujjal Poddar, Surender Kumar Yachha, .Sheo Kumar, #Richa Lal, Anshu Srivastava
Department of Pediatric Gastroenterology, *Radiology and #Pediatric Surgery, SGPGIMS, Lucknow, India
Corresponding Author:
Dr. Ujjal Poddar
E-mail: ujjalpoddar@hotmail.com
48uep6bbphidcol2|ID 48uep6bbphidvals|1710 48uep6bbph|2000F98CTab_Articles|Fulltext Though there are clear-cut guidelines for the management of blunt trauma to the abdomen in children, the management of post-traumatic pseudo-aneurysm of the liver remains controversial.[1] Some people believe that prophylactic angiographic embolization should be done in all cases of post-traumatic liver pseudo-aneurysm because of risk of catastrophic bleeding while others believe that they can just be observed as spontaneous resolution is known to occur. Here, we report the case of a 7-year old child who had a post-traumatic pseudo-aneurysm of the left hepatic artery that resolved spontaneously.
Case Report
A 7-year-old girl presented with abdominal distension and pain for 5 days following blunt trauma to her abdomen. She was hit by a metal box which fell on her abdomen from a height of around 5 feet. There was no history of hematemesis or melena. The child was hemodynamically stable. Her abdominal examination revealed mild distension with tenderness over the epigastrium. She did not have ascites, any palpable lump or any feature of pneumoperitoneum.
Investigations showed normal complete blood counts (Hb: 11.4 g/dL, TLC: 7,900, Platelets: 1.6 x 105/mm3); liver function tests were within normal limits and so was serum amylase.
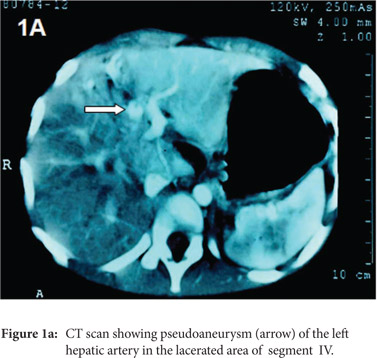
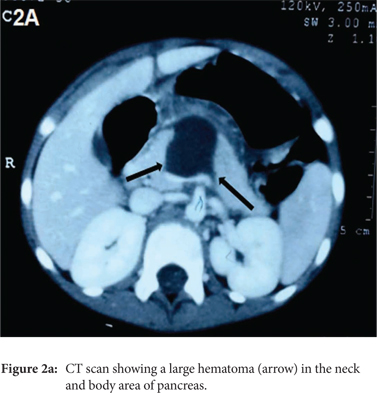
CT-scan abdomen (on the day 6 following trauma) showed a heterogeneous lesion in the liver extending up to the surface, measuring 2.8×2.3×2.4cm and involving segment IVa and IVb which was suggestive of a liver laceration. A focal area (13.3×10.3mm) of staining in arterial phase with enhancement in portal and venous phase was seen in the laceration which was suggestive of a pseudo-aneurysm of the left hepatic artery (Figure 1A). Also, there was a hematoma (3.2× 2.9 ×2.8 cm) at the junction of the neck and body of the pancreas (Figure 2A). Other abdominal viscera were normal.
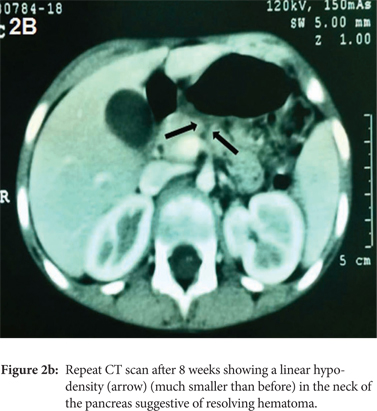
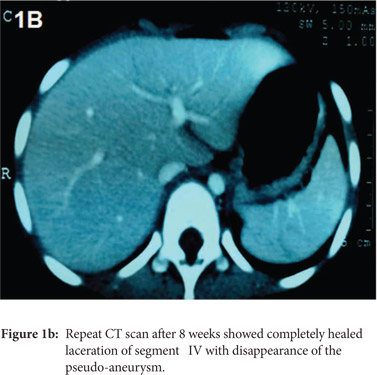 As the child remained hemodynamically stable and there was no further pain, distension or fall in haemoglobin, she was managed conservatively and followed up with weekly Doppler ultrasound to monitor the size of the pseudo-aneurysm. Over the following two weeks, the size of the pseudo-aneurysm remained static and there were no signs of rupture. By the third week, the size reduced with no flow detected in the pseudo-aneurysm and by the fourth week, it resolved completely. A repeat CT-scan was done after 8 weeks in which no pseudo-aneurysm could be seen (Figure 1B). Although there was complete resolution of the liver laceration, a linear hypo-density (much smaller than before) persisted in the neck of the pancreas, which suggested that the haematoma was resolving (Figure 2B). On follow-up over the following 3 months, the child remained asymptomatic.
As the child remained hemodynamically stable and there was no further pain, distension or fall in haemoglobin, she was managed conservatively and followed up with weekly Doppler ultrasound to monitor the size of the pseudo-aneurysm. Over the following two weeks, the size of the pseudo-aneurysm remained static and there were no signs of rupture. By the third week, the size reduced with no flow detected in the pseudo-aneurysm and by the fourth week, it resolved completely. A repeat CT-scan was done after 8 weeks in which no pseudo-aneurysm could be seen (Figure 1B). Although there was complete resolution of the liver laceration, a linear hypo-density (much smaller than before) persisted in the neck of the pancreas, which suggested that the haematoma was resolving (Figure 2B). On follow-up over the following 3 months, the child remained asymptomatic.
 Discussion
Post-traumatic pseudo-aneurysm of the liver is an uncommon but potentially dangerous sequel of blunt trauma abdomen. In a recent series of 176 cases of abdominal trauma in children, 3 had developed pseudo-aneurysm (1.7%) and all of them were associated with grade IV liver injuries (3 of 11 or 27% of grade IV injuries).[2] Two had life-threatening hemorrhage which was controlled by angiographic embolization in one and by laparotomy in the other while the asymptomatic patient underwent prophylactic angiographic embolization. There is a report of hemorrhagic shock in a 14-year old child with post-traumatic hepatic pseudo-aneurysm rupture which was successfully managed by embolization.[3] Sidhu et al reported three children with post-traumatic hepatic pseudoaneurysms.[4] Though only one child had bleeding into the gastrointestinal tract, all three underwent angiographic embolization. In a recent case report, Yi et al did a prophylactic embolization of a post-traumatic hepatic artery pseudo-aneurysm in a 10-year-old-child.[5]
There is no consensus on the issue of managing post-traumatic pseudo-aneurysm of the liver detected on routine follow-up imaging as the natural history of these lesions has not yet been defined. Many people prefer to manage these cases with prophylactic angiographic embolization as the technique and success of angiographic embolization are quite satisfactory and there is a risk of catastrophic bleeding following rupture of the pseudo-aneurysm. However, this approach is more often a panic-driven reaction than one based on firm evidence.
Spontaneous resolution of post-traumatic pseudo-aneurysm of the hepatic artery is possible and usually happens early in the course. In a report of a 4-year-old girl, who sustained blunt trauma to the abdomen and was detected to have 3 pseudo-aneurysms of the liver on day 7, angiographic catheter embolization was not done due to nonmedical issues, and she was followed up radiologically. Partial thrombosis of the pseudo aneurysm was documented in the second week and complete resolution by 6 weeks.[6] Similarly, in a study of 186 children with traumatic splenic injury, 7 of 10 splenic artery pseudo-aneurysms thrombosed spontaneously within 12 days of the injury.[2] In our case also, partial thrombosis of the pseudo-aneurysm was documented in the third week and complete resolution occurred by 4 weeks. Hence, an incidentally detected hepatic artery pseudo-aneurysm following trauma can be safely observed for 2 to 4 weeks and if there are no signs of thrombosis after 4 weeks, prophylactic embolisation may be considered.
References
Discussion
Post-traumatic pseudo-aneurysm of the liver is an uncommon but potentially dangerous sequel of blunt trauma abdomen. In a recent series of 176 cases of abdominal trauma in children, 3 had developed pseudo-aneurysm (1.7%) and all of them were associated with grade IV liver injuries (3 of 11 or 27% of grade IV injuries).[2] Two had life-threatening hemorrhage which was controlled by angiographic embolization in one and by laparotomy in the other while the asymptomatic patient underwent prophylactic angiographic embolization. There is a report of hemorrhagic shock in a 14-year old child with post-traumatic hepatic pseudo-aneurysm rupture which was successfully managed by embolization.[3] Sidhu et al reported three children with post-traumatic hepatic pseudoaneurysms.[4] Though only one child had bleeding into the gastrointestinal tract, all three underwent angiographic embolization. In a recent case report, Yi et al did a prophylactic embolization of a post-traumatic hepatic artery pseudo-aneurysm in a 10-year-old-child.[5]
There is no consensus on the issue of managing post-traumatic pseudo-aneurysm of the liver detected on routine follow-up imaging as the natural history of these lesions has not yet been defined. Many people prefer to manage these cases with prophylactic angiographic embolization as the technique and success of angiographic embolization are quite satisfactory and there is a risk of catastrophic bleeding following rupture of the pseudo-aneurysm. However, this approach is more often a panic-driven reaction than one based on firm evidence.
Spontaneous resolution of post-traumatic pseudo-aneurysm of the hepatic artery is possible and usually happens early in the course. In a report of a 4-year-old girl, who sustained blunt trauma to the abdomen and was detected to have 3 pseudo-aneurysms of the liver on day 7, angiographic catheter embolization was not done due to nonmedical issues, and she was followed up radiologically. Partial thrombosis of the pseudo aneurysm was documented in the second week and complete resolution by 6 weeks.[6] Similarly, in a study of 186 children with traumatic splenic injury, 7 of 10 splenic artery pseudo-aneurysms thrombosed spontaneously within 12 days of the injury.[2] In our case also, partial thrombosis of the pseudo-aneurysm was documented in the third week and complete resolution occurred by 4 weeks. Hence, an incidentally detected hepatic artery pseudo-aneurysm following trauma can be safely observed for 2 to 4 weeks and if there are no signs of thrombosis after 4 weeks, prophylactic embolisation may be considered.
References
- Stylianos S. Evidence-based guidelines for resource utilization in children with isolated spleen or liver injury. The APSA Trauma Committee. J Pediatr Surg. 2000; 35: 164-9.
- Safavi A, Beaudry P, Jamieson D, Murphy JJ. Traumatic pseudoaneurysms of the liver and spleen in children: is routine screening warranted? J Pediatr Surg. 2011; 46: 938–41.
- Hacker HW, Schwobel MG, Allgayer B. and his aPTT was 50.4 seconds; corrected to 30.4s Pseudoaneurysm rupture after liver injury in a 14- with ½ patient and ½ control serum. CT angiogram year old boy. Eur J Pediatr Surg. 2008; 18: 126-8.
- Sidhu MK, Shaw DW, Daly CP, Waldhausen JH, Coldwell D. Post-traumatic hepatic pseudoaneurysms in children. Pediatr Radiol. 1999; 29: 46-52.
- Yi IK, Miao FL, Wong J, Narasimhan KL, Lo RHG, Yee L, et al. Prophylactic embolization of hepatic artery pseudoaneurysm after blunt abdominal trauma in a child. J Pediatr Surg. 2010; 45: 837-9.
- Soudack M, Epelman M, Gaitini D.Spontaneous thrombosis of hepatic post-traumatic pseudoaneurysms: sonographic and computed tomographic features. J Ultrasound Med. 2003; 22: 99–103.
|