Mohammed Amine Benatta, Kellou Naila, Hadjmati Salaheddine, Kezzoula Djamel, Kordjani Slimane, Rebiai Souad, Lagoune Hind, Meddah Abdelaziz
Military Central Hospital Kouba Algiers
Corresponding Author:
Mohammed Amine Benatta
e-mail: benattaamine@yahoo.fr
48uep6bbphidcol2|ID 48uep6bbphidvals|1707 48uep6bbph|2000F98CTab_Articles|Fulltext The first percutaneous endoscopic gastrostomy (PEG) placement in our country, Algeria was reported seven years earlier by our team. Since that first report, only one hundred PEG have been performed. All PEG have been performed with the pull method reported by Gauderer and Ponsky in 1980.[1] The Balloon PEG (BPEG), a balloon-retained tube is often placed as a replacement for PEG. However, they can be placed as an initial tube feeding under endoscopic guidance by the introducertype PEG technique first described by Russell et al. in 1984.[2] This method utilizes the Seldinger technique and requires a specific kit (trocar with peel-away sheet catheter). Recently, given the lack of both pull PEG kits and the peel-away sheet catheter despite the increasing demand, we attempted an initial placement of a BPEG, the only available PEG type. Without a peel-away sheet catheter, we had two challenges: the first one was to create the gastrocutaneous stoma and the second one was to dilate the stoma to introduce our BPEG tube. Necessary equipment for this procedure included a syringe with a small-gauge needle, a scalpel, local anesthetic, a large-gauge puncture needle sheath catheter, a wire, polypectomy snare or foreign body forceps, a reusable 24 Fr pull type PEG tube without external bumper, Savary- Gilliard guide wire, an 18 Fr BPEG (Wilson COOK) and a small caliber endoscope (GIF XP-260; Olympus Optical Co., Ltd., Tokyo, Japan).
Case Report
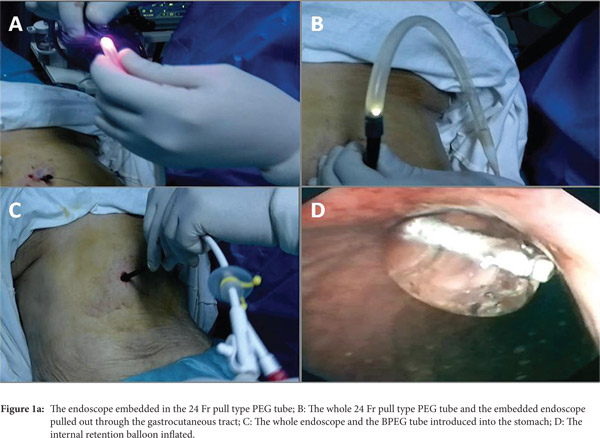
First, a gastrocutaneous tract was created with the classic pull method. The procedure was performed after prior fasting of at least 6 h, under strict aseptic conditions, and antibiotic prophylaxis. The patient was positioned supine, under mild sedation. Two operators were required to create the gastrocutaneous stoma: one performed the endoscopy while the second worked from the abdominal site. After maximal air insufflations, the exact site of the PEG insertion was determined by gastroscopic transillumination using the small caliber endoscope orally inserted and with finger indentation. The abdominal wall was cleaned with disinfectant and an incision was made under local anesthesia. The puncture needle was inserted through the incision into the stomach cavity under endoscopic guidance. Next, a wire was inserted into the stomach through the outer sheath of the puncture needle, grasped by a snare or a foreign body forceps, and pulled out by the endoscope through the mouth. The endoscope was than embedded in the pull type PEG tube without external bumper (Figure 1A). The whole PEG tube and the embedded endoscope was attached to the wire and pulled out through the gastrocutaneous tract creating and dilating the gastrocutaneous stoma (Figure 1B). Then the transgastrostomic endoscope was dis-embedded from the PEG tube. A Savary-Gilliard guide wire was then pushed through the scope to the cutaneous side and inserted in a BPEG. Simultaneously, the whole endoscope and BPEG tube on the metallic guide wire was pushed from the cutaneous side and pulled out through the mouth. Under direct endoscopic view, the BPEG was introduced into the stomach (Figure 1C) and the internal retention balloon inflated with the prefilled syringe (20 cc) (Figure 1D). Finally, the endoscope and the Savary-Gilliard guide wire were pulled out.
A total of 4 procedures of initial placement of BPEG tube were successfully performed in 4 patients. The
classic introducer-type PEG technique requires smaller diameter feeding tubes, resulting in more frequent occlusion and dislodgement which may be reduced by the use of gastropexy. The use of a transgastrostomic endoscope was reported for percutaneous endoscopic jejunostomy placement and was inserted through a mature gastrocutaneous tract from the abdominal side.[3-6] Initial placement of BPEG using a transgastrostomic endoscope is easy and safe and should be attempted even in cases without a previous stoma. This method allows immediate enteral access and may be extended as an initial placement to all types of PEG tube replacement.
References
- Gauderer MW, Ponsky JL, Izant Jr RJ. Gastrostomy without laparotomy: a percutaneous endoscopic technique. J Pediatr Surg. 1980;15:872–5.
- Russell TR, Brotman M, Norris F. Percutaneous gastrostomy. A new simplified and cost-effective technique. Am J Surg. 1984;148:132–7.
- Chaurasia OP, Chang KJ. A novel technique for percutaneous endoscopic gastrojejunostomy tube placement. Gastrointest Endosc. 1995;42(2):165-168.
- Baron TH. Direct percutaneous endoscopic jejunostomy through a mature gastrostomy tract.Gastrointest Endosc. 2002;56:946-947.
- Adler DG, Gostout CJ, Baron TH. Percutaneous transgastric placement of jejunal feeding tubes with an ultrathin endoscope. Gastrointest Endosc. 2002;55:106-110
- Nishiwaki S, Araki H, Shirakami Y, Kawaguchi J. Direct percutaneous endoscopic jejunostomy using a transgastrostomic endoscope in patients with previous endoscopic gastrostomy. Endoscopy. 2009;41(S 02),E36-E37.
|