48uep6bbphidcol2|ID
48uep6bbphidvals|1705
48uep6bbph|2000F98CTab_Articles|Fulltext
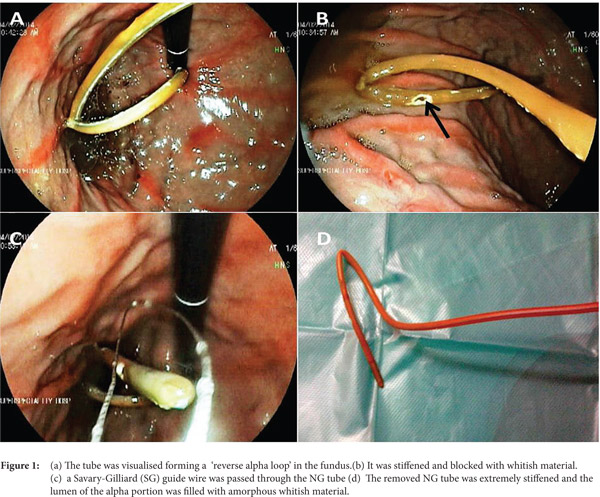
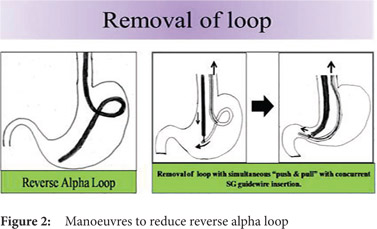
The nasogastric (NG) tube is used extensively in medical practice for the purpose of feeding and gastric decompression. Despite the many uses of the NG tube, its insertion and prolonged presence are not without complications. Necrosis of the nasal ala and the NG tube syndrome wherein there is ulceration and infection of the posterior cricoid region with subsequent dysfunction of vocal cord abduction are some complications which have been documented.[1] Although NG tube coiling and knotting is a known complication, it is more commonly seen with small-diameter tubes or in patients with a small stomach such as following gastroplasty.[1] Insertion of an excessive length of the NG tube into the stomach, endotracheal intubation and repetitive advancement of the tube are the other risk factors associated with knotting of the tube. Pushing or pulling of the NG tube after it has been placed-either by the operator or due to coughing or neck movement-may lead to the formation of a loop.[2] Most previous case reports on NG tube knotting have described tubes that were left in-situ for prolonged durations, ranging from 1 to 12 days.[1] Looping of small-bore feeding tubes and NG tubes during insertion is common; however, forming a stiffened and irreversibly fixed loop due to internal solidification by feeding formula is a rare complication.We hereby report a case of prolonged NG feeding with stiffened and fixed looped NG tube in the stomach that was difficult to remove when the patient was considered for percutaneous endoscopic gastrostomy (PEG) tube placement. One is therefore compelled to share this experience in order to alert clinicians about this complication which may be encountered during the use of this simple and widely used tube in clinical practice.Case ReportAn 84-year old male who was diabetic, hypertensive and a known case of obstructive airway disease developed a stroke one-and-a-half months back. He was put on 14 Fr NG feeding due to oropharyngeal dysphagia and nasal regurgitation. The patient also underwent a tracheostomy. He was given casein-based formula feeds, sucralfate and other medications through the NG tube. He was referred to the gastroenterology department for placement of a PEG tube due to recent inability to feed through the NG tube. When we tried to remove the NG tube it seemed to be stuck up at approximately the 50cm mark. During endoscopy, an adult gastroscope could not be passed across the cricopharynx due to the relative narrowing caused by the indwelling NG tube along with compression produced by the tracheostomy tube. A paediatric scope was successfully passed across with some difficulty. The tube was visualised forming a fixed and irreducible ‘reverse alpha loop’ in the fundus. It was stiffened and blocked with whitish material. When it was pulled up, the stiffened fixed loop was seen to be getting obstructed at the GE junction (Figure 1). Attempts to cut the tube with snare and cautery and remove it piecemeal also failed. Thereafter, a Savary-Gilliard (SG) guide wire was passed through the NG tube up to the beginning of the loop after encountering some resistance. The distal end of the loop was grasped with a snare and the nasal end of the NG tube was pulled simultaneously with further advancement of the SG guide wire through the NG tube whilst the gastric end of the NG tube held by the snare was pushed along with the scope towards the pylorus. By this maneuver, the loop was removed and the NG tube was straightened and kept in the same position by the SG guide wire (Figure 2). The tube was removed slowly with the guide wire in-situ. The endoscopy was then completed and was unremarkable except for a small hiatus hernia and mild esophagitis and gastritis. The patient underwent a PEG safely the next day. The removed NG tube was extremely stiffened and the lumen of the alpha portion was filled with amorphous whitish material.
 DiscussionNG tube feeding is a very common modality used to maintain the nutritional status of patients who are unable to take food orally. However, this simple tube can rarely cause complications including a few serious ones. The reported complication rates range from 0.3% to 8%.[1] NG tube looping, knotting and impaction are amongst the rare complications.[3] The NG tube can coil back on itself forming a loop or a knot when an excessive length of the tube is introduced into the stomach; however, the reported incidence of this is low.[4] Risk factors associated with looping and knotting of the NG tube are small bore tubes, patients with small stomachs, insertions of excessive length of the NG tube into the stomach, repetitive advancement of the tube and endotracheal intubation.[1] Loop formation may occur as a result of excessive manipulation of the NG tube after being placed, either by medical personnel or due to coughing or neck movement of patient.[2] It is also necessary to measure the appropriate NG tube length to be placed so that only the necessary length of the tube is inserted and any unrecognized tube movement can be detected.[1] This is done by measuring from the nostril along the side of the face past the ear and up to the xiphisternum and marking this length on the tube with a marker or a tape. The possibility of NG tube knotting should be kept in mind if a resistance is felt during its attempted removal. It can be confirmed by a plain x-ray or a film with water soluble contrast rendered via the NG tube.[1]References
DiscussionNG tube feeding is a very common modality used to maintain the nutritional status of patients who are unable to take food orally. However, this simple tube can rarely cause complications including a few serious ones. The reported complication rates range from 0.3% to 8%.[1] NG tube looping, knotting and impaction are amongst the rare complications.[3] The NG tube can coil back on itself forming a loop or a knot when an excessive length of the tube is introduced into the stomach; however, the reported incidence of this is low.[4] Risk factors associated with looping and knotting of the NG tube are small bore tubes, patients with small stomachs, insertions of excessive length of the NG tube into the stomach, repetitive advancement of the tube and endotracheal intubation.[1] Loop formation may occur as a result of excessive manipulation of the NG tube after being placed, either by medical personnel or due to coughing or neck movement of patient.[2] It is also necessary to measure the appropriate NG tube length to be placed so that only the necessary length of the tube is inserted and any unrecognized tube movement can be detected.[1] This is done by measuring from the nostril along the side of the face past the ear and up to the xiphisternum and marking this length on the tube with a marker or a tape. The possibility of NG tube knotting should be kept in mind if a resistance is felt during its attempted removal. It can be confirmed by a plain x-ray or a film with water soluble contrast rendered via the NG tube.[1]References
- Awe JAA. Self knotting of Nasogastric tube: An unusual and rare complication. Global Advanced Research Journal of Microbiology. 2014; 3(4):64-7.
- Agarwal A, Gaur A, Sahu D, Singh PK, Pandey CK. Nasogastric tube knotting over the epiglottis: A cause of respiratory distress. Anesth Analg. 2002; 94:1659-60.
- Liao GS, Hsieh HF, Wu MH, Chen TW, Yu JC, Liu YC. Knot formation in the feeding jejunostomy tube: a case report and review of the literature. World J Gastroenterol. 2007; 13:973-4.
- Dasani B, Sahdev P. Knotting of a nasogastric tube: a case report. Am J Emerg Med. 1991; 9(6):565.