48uep6bbphidcol2|ID
48uep6bbphidvals|1702
48uep6bbph|2000F98CTab_Articles|Fulltext
Chromhidrosis is the production of colored sweat by eccrine or apocrine sweat glands. Pseudochromhidrosis is the production of colourless sweat, which then becomes coloured when it reaches the skin and combines with agents like chromogenic bacterial products (such as those produced by species of corynebacteria) , certain chemicals, paints and dyes. Only a few cases have been reported previously.[1,2] Here, we report the case of a 25-year old male with pseudochromhidrosis who was earlier diagnosed with celiac disease and dermatitis herpetiformis.
Case report
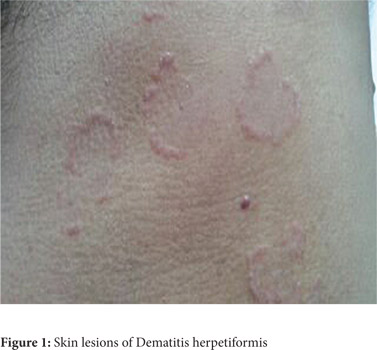
A 25-year old male was referred to the Gastroenterology OPD with presenting complaint of yellowish discoloration of sweat for the last one month. He had consulted many physicians before reaching us. He was on a glutenfree diet. There was no icterus, peripheral oedema or organomegaly. Six months ago, he was diagnosed as a case of celiac disease with dermatitis herpetiformis and was under treatment elsewhere for the same (Figure 1).
On examination, his underclothes had deep yellow stains in the axilla, chest, back and groin (Figure 2).His workup including blood counts, liver function tests, urine routine microscopy, urine homogentisic acid, ultrasound scan of the abdomen and skin biopsy were unremarkable. He was diagnosed as a case of pseudochromhidrosis and treated with oral ciprofloxacin and erythromycin for 4 weeks to which the patient responded well.
 Discussion
Discussion
Both chromhidrosis and pseudochromhidrosis are rare. The diagnosis of chromhidrosis is based on biopsy and autofluorescence of skin specimens and stained clothing, while the diagnosis of pseudochromhidrosis is based primarily on history and a good response to treatment with antibiotics[1]. Oxidized lipofuscins, which autofluoresce at 360 nm, have been detected by examining stained clothing with ultraviolet light and by autofluorescence microscopy of skin biopsies[2].
Treatment options for chromhidrosis is limited. Capsaicin depletes the neurons of substance P and has been found to be beneficial in the treatment of these patients. The other options are topical clindamycin and topical aluminum chloride. The definitive treatment is surgical excision of the apocrine sweat glands[3]. In contrast to chromhidrosis, pseudochromhidrosis is easily treatable[4]. Pseudochromhidrosis due to bacterial causes can be treated with systemic and topical antibiotics. Pseudochromhidrosis due to exogenous dyes, paints or other chemicals can be remedied by avoiding these compounds.
References
- Cilliers J, de Beer C. The Case of the Red Lingerie –Chromhidrosis Revisited. Dermatology. 1999; 199:149-52.
- Cox NH, Popple AW, Large DM. Autofluorescence of clothing as an adjunct in the diagnosis of apocrine chromhidrosis. Arch Dermatol. 1992; 128:275-6.
- Marks JG. Treatment of apocrine chromhidrosis with topical capsaicin. J Am Acad Dermatol. 1989; 21:418-20.
- Singal A, Thami GP. Red pseudochromhidrosis of the neck. Clin Exp Dermatol. 2004: 29;548-9.