Mitul B Kalathia1, Yagnesh Popat2, Jagdish Prasad Goyal1
Department of Pediatrics1,
All India Institute of Medical Sciences,
Rishikesh.
PDU Govt. Medical College, Rajkot
Om Baby care Hospital2
Corresponding Author:
Dr Jagdish Goyal
Email: jpgoyal@rediffmail.com
48uep6bbphidvals|1348 48uep6bbphidcol2|ID 48uep6bbph|2000F98CTab_Articles|Fulltext Johanson Blizzard syndrome (JBS) was described in 1971 by Johanson & Blizzard.[1] It is an autosomal recessive disorder characterized by exocrine pancreatic insufficiency, absent or hypoplastic alae nasi, ectodermal scalp defect, microcephaly, congenital deafness and growth retardation.[2,3] Only two cases have been reported in the literature from India till date.[4,5] We here report a rare case of JBS who presented to us with chronic diarrhoea and failure to thrive.
Case History
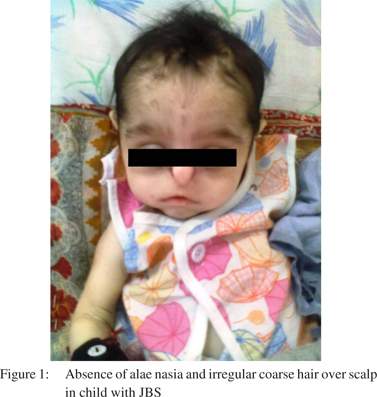
A 5-months old female child presented to us with a history of not gaining weight accompanied by diarrhoea since the neonatal period. She also had history of pedal edema over the past two months. The child was born out of consanguineous marriage and previously male child with dysmorphism had expired during the neonatal period. The birth history was uneventful, patient cried immediately after birth and her birth weight was 2.8 kg. She had global developmental delay. On physical examination, the child was lethargic with poor muscle tone and had severe pallor. Her weight was 2.9 kg (< 3rd percentile), length was 49 cm (< 3rd percentile) and head circumference was 34 cm (< 3rd percentile) suggestive of microcephaly. Her anterior fontanel was wide open. There was absence of alae nasi, parrot beak nose, low set ear, patchy alopecia with irregular coarse hair over scalp (Figure 1). Pitting edema was also detected feet on physical examination. Investigations revealed Hb 4.2 g/dL, WBC 17.1×103/µL, platelets 208×103/µL, CRP 11.4 mg/L, ALT 45U/L, AST 32U/L, bilirubin 0.8 mg/dL, protein 4.8 g/dL, albumin 2.3 g/dL, urea 11 mg/dL, creatinine 1.1 mg/dL, Na 149 mEq/L, K 3.1mEq/L and Ca 7.5 mg/dL. Serum amylase and lipase were low. Thyroid function test showed low T4 and elevated TSH suggestive of hypothyroidism. Whole body X-ray, USG abdomen, CT scan brain and echocardiography were normal. Genetic study and BERA were not performed, as the parents were neither willing nor could afford the same. She was treated with antibiotics, and thyroxin supplementation, with plan to start pancreatic supplementation. The patient was discharged against medical advice on the 3rd day of admission and died at home as confirmed telephonically.
Discussion
The most common complication of JBS is malabsorbtion syndrome due to exocrine pancreatic insufficiency, which may lead to chronic diarrhoea, anaemia, hypoproteinemia, oedema and infection, ultimately causing death.[6] There is no definitive treatment for JBS. Management of JBS is symptomatic and supportive.
JBS can be diagnosed early by antenatal USG detecting aplasia of alae nasi in suspected couples of consanguineous marriage.[7] Early diagnosis helps in timely management of pancreatic insufficiency and hypothyroidism. The present case highlights the importance of genetic counselling and antenatal diagnosis as this syndrome is autosomal recessive and chances of recurrence are 25% in subsequent offerings.
References
- Johanson A, Blizzard R. A syndrome of congenital aplasia of the alae nasi, deafness, hypothyroidism, dwarfism, absent permanent teeth, and malabsorption. J Pediatr. 1971;79:982–7.
- Almashraki N, Abdulnabee MZ, Sukalo M, Alrajoudi A, Sharafadeen I, Zenker M. Johanson-Blizzard syndrome. World J Gastroenterol. 2011;17:4247–50.
- Ramos S, Ramos HF, Ramos RF, Peixoto CA, Ramos BF. Johanson-Blizzard syndrome. Braz J Otorhinolaryngol. 2010;76:794.
- Kulkarni ML, Shetty SK, Kallambella KS, Kulkarni PM. Johanson—blizzard syndrome. Indian J Pediatr. 2004;71:1127–9.
- Sudarshan R, Annigeri RG, Shettar SS. Johanson –Blizzard Syndrome: A rare case report. Journal of Indian Academy of Oral Medicine and Radiology. 2010;22:225–8.
- Hoffman WH, Lee JR, Kovacs K, Chen H, Yaghmai F. Johanson-Blizzard syndrome:autopsy findings with special emphasis on hypopituitarism and review of the literature. Pediatr Dev Pathol. 2007;10:55–60.
- Vanlieferinghen P, Gallot D, Francannet Ch, Meyer F, Dechelotte P. Prenatal ultrasonographic diagnosis of a recurrent case of Johanson-Blizzard syndrome. Genet Couns. 2003;14:105–7.
|