Introduction
Acute liver failure (ALF) is caused by rapid loss of hepatocytes along with development of encephalopathy without antecedent liver illness.1 Management of ALF, a disease with a rapid downhill course, has undergone a paradigm shift with the advent of liver transplantation as a treatment option. However, prognostication and triage at an early stage is important to identify those patients who could be maximally benefitted from a timely transplant.
There are various established prognostication models in the Western literature, having varying sensitivity and specificity.2-7 However, when applied to ALF patients in Asian countries, these models lose the diagnostic accuracy, mostly because of the fact that the etiology of ALF in Asian countries (viral etiology) is very much different from that of the West (acetaminophen overdose).8-10 Hence, there is a definite necessity to find a specific, and early marker of mortality in a cohort of ALF patients from this part of the world.
In a patient of ALF, loss of hepatocytes may be caused by apoptosis and necrosis. There are varying evidences regarding relative importance of apoptosis and necrosis in ALF patients. Apoptosis is mediated by caspases which are intracellular cysteine proteases that cleave various proteins including cytokeratin (CK) 18, an intermediate filament, responsible for maintaining the cytoskeletal structure in the liver and other epithelial cells. Hepatocyte apoptotic cell death is associated with the release of caspase-cleaved CK18 (CK18)11, whereas intact full length CK18 is released from cells undergoing necrosis.12 Hence, measurement of caspase-cleaved cytokeratin (CK)-18 can indicate the extent of apoptotic cell death in ALF patients.13-15 The M30 ELISA, a sandwich ELISA, measures the caspase cleaved CK18 released during apoptosis.16
In the light of few studies with regard to cell death markers, and their role in prognostication of ALF patients, we conducted this study to assess the role of CK 18 (M30) in ascertaining the prognosis of patients with Acute Liver failure. This will likely help in identifying those who are in definite need for liver transplant from those who would survive with conservative managment.
Methods
Patients
Our study evaluated 45 patients fulfilling our criteria for ALF. Before enrolling patients, ethical clearance was obtained from the ethics department of the institute, and consent was taken from patient’s nearest relative. For the purpose of the study, inclusion criteria for ALF was taken as INR>1.5, altered mental status without any antecedent liver illness, and duration of disease <8 weeks.17 Patients having autoimmune hepatitis or suspected drug induced liver disease were excluded from analysis.
Management Protocol
All patients were managed in intensive care unit with a uniform management protocol that included stress ulcer prophylaxis, glycaemic control, and elective ventilation for patients with grade IV encephalopathy or grade III encephalopathy with cerebral oedema. The fluid resuscitation was carried out with crystalloid, with the aim to maintain central venous pressure around 10 cm of saline. Vasopressor (noradrenaline) was started when systemic hypotension persisted despite correction of volume status, and the goal was to maintain a mean arterial pressure =60 mm Hg. Intravenous mannitol was used to control cerebral oedema. Prophylactic antibiotics with daily microbiological surveillance were used to detect infection. Renal replacement therapy (haemodialysis) was utilised for refractory metabolic acidosis, severe hyperkalemia and fluid overload.
Biochemical Analysis
All patients were subjected to liver function evaluation (utilising AST, ALT, alkaline phosphatase, serum bilirubin). In addition, serum creatinine and coagulation profile was obtained. Through these variables, MELD was calculated to assess severity of the disease. Hepatitis viral markers for HAV (IgM anti- HAV), HBV (HBsAg and IgM HBcAb), HCV (anti-HCV) and HEV (IgM anti-HEV) were measured to assess active infection.
Estimation of CK 18 M30
CK 18 M30 levels were measured twice (day of admission, and day 3/last sample day in case of expiry before 3 days) using Human Cytokeratin 18-M30 (CK 18-M30) ELISA Kit (Catalog Number.CSB-E13696h) manufactured by Cusabio technology.
Statistical Analysis
A p value lesser than 0.05 was considered statistically significant. Statistical analysis was performed using SPSS ver. 20. Chi square test or Fischer’s test were utilized to analyze categorical data. Quantitative data was assessed on mean± standard deviations, and Student’s t-test was used to aid in data analysis. In addition, Receiver Operating Characteristic (ROC) curve was used to analyze data. To construct a prediction model, a univariate screening of covariates was done and significant covariates (p < 0.5) were used in the regression model for the prediction of outcomes.
Results
Baseline Characteristics and Predictors of Outcome in Acute Liver Failure Patients
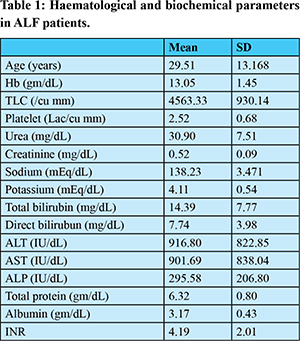
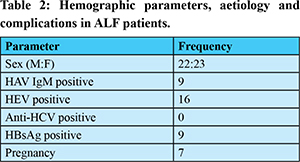
The demographic, clinical and laboratory characteristics of 45 ALF patients are depicted in Tables 1 and 2. With medical treatment, 36 patients (80%) died, and 9 patients (20%) survived. HEV was found to be the commonest cause of ALF accounting for 35.55% of ALF patients. HAV was the second most common virological agent identified in ALF group causing 20 % of all cases. The mean duration of illness in those who survived was 7 (± 0.76) days from onset of symptoms and 9 (± 0.54) days in the non-survivor group.
The mean cleaved CK18 [M30] levels in ALF patients who survived were 767.37±247.97mIU/ml and in those who died were 1094.67±239.37mIU/ml. The difference in values between these groups was statistically significant (p=0.004). A receiver operating characteristic curve was drawn for serum CK 18(M30) levels (Figure 1). The area under the curve was 0.809. A cut-off level of =988.07 mIU/ml was found to predict mortality with 69.4% sensitivity and 77.8% specificity. It had a positive predictive value of 100%, a negative predictive value of 39.1% and a diagnostic accuracy of 68.9%.
It was also found that in univariate analysis between the groups of patients that survived and died, there was statistically significant difference in total leucocyte count, serum creatinine, INR and cleaved CK18 (M30) levels (Table 3).
A multivariate analysis was performed using these variables, and it was found that variables that independently predicted mortality were INR (OR, 1.077; 95% CI, 1.033-1.123), total leukocyte count (OR, 1.2; 95% CI, 1.09-1.054) and cleaved CK18 [M 30] levels at day 1 of admission (OR, 1.34; 95% CI, 1.12-1.58)
The predicted probability of mortality can be found from the equation:
COMPUTED SCORE= -0.404 + (0.074*INR) + (0.00004513*TLC) + (0.0001*M30)
This score was calculated for all ALF patients, and the value of this score was significantly higher in the patients who died compared with the patients who survived.
A receiver operating characteristic curve was drawn for this new score (Figure 2). The area under the curve was 0.978. A cut-off level of =0.157 was found to predict mortality with 94.4% sensitivity and 89.9% specificity. It had a positive predictive value of 94.4%, a negative predictive value of 77.7% and a diagnostic accuracy of 91.1%.
King’s College Hospital Criteria
King’s college hospital criteria for non-paracetamol induced ALF were used to find out the patients having poor outcome. KCH was found to predict mortality with 60% sensitivity and 85.7% specificity. It had a positive predictive value of 93.75%, a negative predictive value of 37.5% and a diagnostic accuracy of 65.63%.
MELD score
The mean MELD score in ALF patients who survived were 15.24±5.91 and in those who died were 36.59±10.59. The difference in values between these groups was statistically significant.
A receiver operating characteristic curve was drawn for MELD scores (Figure 3). The area under the curve was 0.944. A cut-off level of =20.96 was found to predict mortality with 91.7% sensitivity and 88.9% specificity. It had a positive predictive value of 96.9%, a negative predictive value of 66.7% and a diagnostic accuracy of 88.9%.
Comparison of this New Score with Existing Scoring Systems as Individual Predictor of Mortality
Hence, our new scoring system has higher sensitivity & specificity for mortality compared with other standard prognostic markers in ALF, and it has better diagnostic accuracy as shown in Table 5.
Discussion
The present study was designed to study the role of serum apoptosis marker [CK 18(M30)] as early prognostic marker while predicting the course of acute liver failure patients. Acute liver failure is a disease with stormy progression and poor outcome. However, a timely liver transplant can cause substantial increase in the chance of survival of patients with ALF. On the other hand, liver transplant is a costly procedure and has its own complications. Over the years, several prognostic markers have been utilised, however, none of the currently used criteria have the ideal diagnostic accuracy.
There is a considerable variation in the etiology and clinical presentation of ALF in tropical countries from the western countries.7-10 In consistency with other Indian studies,9,10,18 our study revealed HEV as the commonest cause of ALF. Thirty six of the 45 (80%) ALF patients died. The high mortality is owed to lack of liver transplantation facility, and limited ventilator support at our institution. This further emphasizes the need of early and emergent therapeutic interventions in these patients, which highlights the necessity of development of various tools which can accurately predict the severity of this dreadful condition leading to better patient management and improved survival.
Our study elucidates that initial CK 18(M30) levels can predict the outcome in ALF patients.
The data is consistent with previous reports showing that those ALF patients with highest levels of CK 18(M30) had poor prognosis.
Although the presently used criteria for predicting prognosis have good sensitivity and specificity, however, they are able to do so when a high proportion of patients have progressed to advanced liver and multi-organ failure, rendering them unsuitable candidates for liver transplantation.
We also have developed a score to predict outcome in ALF patients at admission. When compared to King’s College Criteria and MELD score, our new predictive model has higher specificity (100%) with a cut-off of 0.34. Accordingly, we suggest that ALF patients with serum Cleaved CK 18[M30] levels at admission more than 988.07mIU/ml are candidates for liver transplantation, which can be life saving for these patients. However, we need to validate this score in a larger group of ALF patients.
Bechmann et al13 and Rutherford et al19 showed in their studies that M30 levels were significantly high in ALF patients. Also the levels of M30 were significantly higher in non-survivor group compared to the survivor group. This is in concordance with the results demonstrated in our study. In contrast Craig et al20 (2011) found that although M30 levels were significantly high in the ALF group; however its level in non-survivor group was not significantly increased compared to those who survived. In another study by Volkmann et al10 (2008), it was inferred that M30 levels were high in ALF patients compared to healthy control. However, it was seen that M30 levels were significantly higher in the survivor group compared to the non-survivor group & it was hypothesized that increased caspase activation is associated with spontaneous recovery. This is contrary to the results of our study. The limitations of our study includes lower sample size and inadequate liver transplantation services which can affect the results from the resource rich settings. CK18 has been identified as a prognostic marker in liver cirrhosis21. Our study highlights the importance of CK18 in acute liver failure and role of the biomarker in prognostic assessment.
Conclusions
CK 18 (M30) is associated with mortality in ALF patients. Prognostic equations utilizing CK18 has potential to predict the mortality and requirement of liver transplant.
Summary Points
1. CK 18 is a useful biomarker to predict and prioritize liver transplant.
2. Modelled equations using CK18 predicts the prognosis better than King’s College criteria and MELD score.
References
- Volkmann X, Anstaett M, Hadem J, Stiefel P, Bahr MJ, Lehner F et al. Caspase activation is associated with spontaneous recovery from acute liver failure. Hepatology 2008;47:1624–33.
- Bernauau J, Rueff B, Benhamaou JP. Fulminant and subfulminant liver failure: definition and causes. Semin Liver Dis 1986;6:97-106.
- Ostapowicz G, Fontana RJ, Schiodt FV, Larson A, Davern TJ, Han SH et al. Results of a prospective study of acute liver failure at 17 tertiary care centers in the United States. Ann Intern Med 2002;137:947–54.
- Sallie R, Silva AE, Purdy M, Smith H, McCaustland K, Tibbs C et al. Hepatitis C and E in non-A non-B fulminant hepatic failure: a polymerase chain reaction and serological study. J Hepatol 1994;20:580-8.
- Lidofsky SD, Bass NM, Prager MC, Washington DE, Read AE, Wright TL et al. Intracranial pressure monitoring and liver transplantation for fulminant hepatic failure. Hepatology 1992;16:1-7.
- Vickers C, Neuberger J, Buckels J, McMaster P, Elias E. Transplantation of the liver in adults and children with fulminant hepatic failure. J Hepatol 1988;7:143-50.
- Schiodt FV, Atillasoy E, Shakil AO, Schiff ER, Caldwell C, Kowdley KV et al. Etiology and outcome for 295 patients with acute liver failure in the United States. Liver TransplSurg 1999;5:29-34.
- Schmidt LE, Dalhoff K. Serum phosphate is an early predictor of outcome in severe acetaminophen-induced hepatotoxicity. Hepatology 2002;36:659-65.
- Acharya SK, Dasarathy S, Kumer TL, Sushma S, Prasanna KS, Tandon A et al. Fulminant hepatitis in a tropical population: clinical course, cause, and early predictors of outcome. Hepatology 1996;23:1448-55.
- Kar P, Budhiraja S, Narang A, Chakravarthy A. Etiology of sporadic acute and fulminant non-A, non-B viral hepatitis in north India. Indian J Gastroenterol 1997;16:43-5.
- Kramer G, Erdal H, Mertens HJ, Nap M, Mauermann J, Steiner G et al. Differentiation between cell death modes using measurements of different soluble forms of extracellular cytokeratin 18. Cancer Res 2004;64:1751–6.
- Yilmaz Y. Systematic review: caspase-cleaved fragments of cytokeratin-18 –the promises and challenges of a biomarker for chronic liver disease. Aliment PharmacolTher 2009;30:1103–9.
- Bechmann LP, Jochum C, Kocabayoglu P, Sowa J, Kassalik M, Gieseler RK et al. Cytokeratin 18-based modification of the MELD score improves prediction of spontaneous survival after acute liver injury. J Hepatology 2010;53:639-47.
- Bechmann LP, Marquitan G, Jochum C, Saner F, Gerken G, Canbay A. Apoptosis versus necrosis rate as a predictor in acute liver failure following acetaminophen intoxication compared with acute-on-chronic liver failure. Liver Int 2008;28:713–6.
- Hofer S, Brenner T, Bopp C, Steppan J, Lichtenstern C, Weitz J et al. Cell death serum biomarkers are early predictors for survival in severe septic patients with hepatic dysfunction. Crit Care 2009;13:R93.
- Olofsson MH, Ueno T, Pan Y, Xu R, Cai F, van der Kuip H et al. Cytokeratin-18 is a useful serum biomarker for early determination of response of breast carcinomas to chemotherapy. Clin Cancer Res 2007;13:3198–206.
- O’Grady JG, Alexander GJ, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology 1989;97:439-45.
- Dhiman RK, Seth AK, Jain S, Chawla YK, Dilawari JB. Prognostic evaluation of early indicators in fulminant hepatic failure by multivariate analysis. Dig Dis Sci 1998;43:1311-6.
- Rutherford AE, Hynan LS, Borges CBS, Forcione DG, Blackard JT, Lin W et al. Serum Apoptosis Markers in Acute Liver Failure: A Pilot Study.ClinGastroenterolHepatol 2007;5:1477–83.
- Craig DGN, Lee P, Pryde EA, Masterton GS, Hayes PC, Simpson KJ.Circulating apoptotic and necrotic cell deathmarkers in patients with acute liver injury.LiverInt 2011;31:1127-36.
- Yang, H., Sun, L., Sheng, L., Wang, X., Xu, H., Du, S., Zhao, H., Lu, X., Sang, X., & Mao, Y. (2017). Serum cytokeratin-18 is a non-invasive biomarker for evaluating disease severity in patients with liver cirrhosis and hepatocellular carcinoma. Translational Cancer Research, 6(6), 1345-1350. doi:10.21037/tcr.2017.12.12.