48uep6bbphidcol2|ID
48uep6bbphidvals|3045
48uep6bbph|2000F98CTab_Articles|Fulltext
Brunner’s gland adenoma (BGA) is a rare and uncommon cause of upper gastrointestinal bleed (UGIB). Brunner’s gland hyperplasia (BGH) accounts for 5% to 10% of benign duodenal tumors, most of these tumours are asymptomatic, but some may present with obstructive symptoms or bleeding, especially if the lesions are larger than 2 cm1. Endoscopic polypectomy is the ideal choice of treatment in small pedunculated lesions. In cases where in endoscopic snaring has failed or the BGA is too large, a surgical excision via duodenotomy may be necessary2 as reported in our case.
Case Report
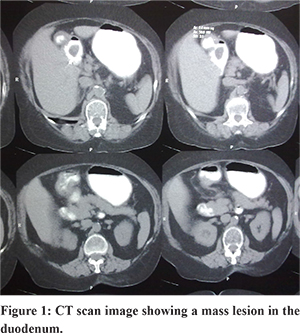
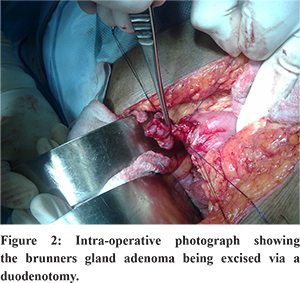
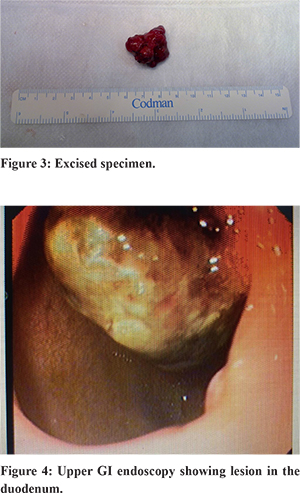
A 65-year-old lady presented to the emergency medicine department with a two hour history of hematemesis and malena. She was hemodynamically stable at the time of examination with no history of NSAID abuse or medical co-morbidities. She was managed conservatively, and an upper gastrointestinal endoscopy done revealed a polyp in the stomach with clots over it and no fresh bleeding. A second endoscopy done after 48 hrs after admission revealed evidence of fresh blood in the duodenum and a duodenal polyp which had intussuscepted into the stomach (Figure 1). She persisted to have melena and despite 4 units of blood transfusion, her hemoglobin levels were dropping. A CT scan done revealed a pedunculated polyp in the first part of duodenum with the pancreas being normal (Figure 2). An attempt at endoscopic polypectomy failed; given her age, on-going melena, dropping levels of hemoglobin, a surgical intervention was planned. She underwent laparotomy, duodenotomy and excision of polyp (Figure 3 & 4). Her recovery was uneventful, and the histopathological examination revealed a Brunner’s gland adenoma.
Discussion
UGIB is commonly secondary to a bleeding duodenal ulcer, BGA is one among the rare causes of UGIB. Curveilhier is credited with reporting the first case of Brunner’s gland adenoma in 18353. Brunner’s gland proliferation less than 1 cm is referred to as Brunner’s gland hyperplasia (BGH) and those more than 1 cm in size in diameter is referred to as Brunner’s gland adenoma (BGA).
BGA tends to affect males and females equally during the fifth or sixth decade. In the series by Levine et al, the adenomas were in the duodenal bulb in 57% of the cases and UGIB was the presenting feature in 37% of the cases4. In patients with a BGA presenting with an UGIB, melena is more common than hematemesis. There can be a life threatening or a fatal bleed. UGIB in BGA is often chronic in nature with anemia as the presenting feature.
The diagnosis of BGA is often difficult and is commonly noticed as an incidental finding. It can present either with features of upper gastrointestinal obstruction or hemorrhage (acute or chronic). The commonest site of affliction is the posterior wall near the junction of first and second parts of duodenum. BGA usually measures 1-4 cm in diameter although adenomas up to 12 cm have been reported in literature. The diagnosis of BGA is often made at endoscopy or on imaging (like a barium meal). Although endoscopy is considered as the gold standard diagnostic modality in BGA, the endoscopic biopsies are often inconclusive because the tumor lies in the sub mucosal layer, which is too deep to be reached by the routine biopsy forceps. The final diagnosis is often made in the post therapy phase on histopathological examination. Although majority of the BGA are benign, dysplastic changes and carcinoma have been reported5.
Once suspected or diagnosed on endoscopy or imaging, early intervention is advocated to avoid the potential complications of UGIB, anemia, duodenal obstruction or intussusception6. Endoscopic or surgical resection is the treatment of choice depending on the size, location, and condition of the patient and availability of resources. In cases where endoscopic approach has failed or is not feasible a surgical localized resection via a duodenotomy or a pancreaticoduodenectomy for extremely large adenomas is necessary7.
References
- Gastrointestinal Endoscopy, Volume 64, Issue 3, September 2006, Pages 464-467
- The American Journal of Surgery, Volume 196, Issue 4, October 2008, Pages e33-e34
- Cruveilhier J. Anatomy of the Human Body. New York: Harper and Bros; 1844
- Levine JA, Burgart LJ, Kbatts KP, Wang KK. Brunner’s gland hamartomas: clinical presentation and pathological features of 27 cases. Am J Gastroent. 1995;90:290–294
- Early primary duodenal carcinoma arising from Brunner’s glands synchronously occurring with sigmoid colon carcinoma: report of a case.Ohta Y - Surg Today - 01-JAN-2008; 38(8): 756-60
- An unusual cause of duodenal obstruction--a case report Selbaková M - Rozhl Chir - 01-JUL-2007; 86(7): 376-
- Surgical management of giant Brunner’s gland hamartoma: case report and literature review. - Stewart ZA - World J Surg Oncol - 01-JAN-2009; 7: 68.