48uep6bbphidcol2|ID
48uep6bbphidvals|2942
48uep6bbph|2000F98CTab_Articles|Fulltext
Spleen is one of the most commonly injured organs following blunt abdominal trauma.1 Spontaneous splenic rupture (SSR) usually occurs in a previously diseased spleen, and non-traumatic rupture of the normal spleen is extremely rare.1 The stress of cough and vomiting, leading to the traumatic rupture of the spleen, is very rare.2 We are reporting a traumatic splenic rupture following vomiting, which was subjected to exploratory laparotomy and splenectomy.
Case Report
A 70-year-old lady was receiving radical radiotherapy with synchronous platinum-based chemotherapy for an oropharyngeal squamous cell carcinoma. After 11 of 30 daily fractions of radiotherapy and a single cycle of carboplatin chemotherapy, she was admitted for nutritional support (nasogastric feeding) and control of acute toxicity of the chemo-radiation, which included nausea and vomiting. During the admission, the retching and vomiting were difficult to control. After ten days, the vomiting worsened and was immediately followed by sudden onset severe pain in the upper abdomen, not radiating to the back. This pain was followed within an hour by clouding of consciousness and drowsiness. There is no history of even trivial trauma preceding this episode except vomiting.
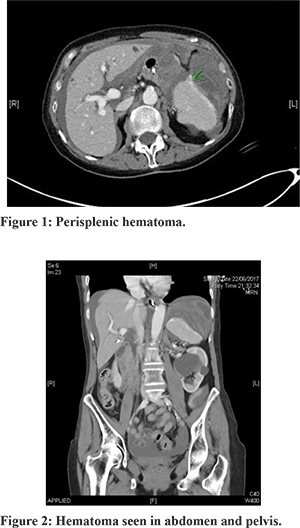
On examination, she was pale and tachycardiac (Pulse rate-100/minute), was sweating, and her blood pressure fell to 60 systolic. On arterial blood gas, haemoglobin fell to 44. The rest of the blood parameters were within normal limits. She was resuscitated with two litres of crystalloid, and a diagnosis of haemorrhagic shock was made. Massive blood loss policy was instigated and transfused three units of blood and one unit platelet. Once stabilized, a Computed Tomography scan (CT) of the abdomen and pelvis with contrast was undertaken to ascertain the exact cause of instability. CT scan showed acute dense hematoma in the left upper quadrant superior to spleen displacing the spleen inferiorly and medially (Figure 1). The hematoma was also seen in the abdomen and pelvis with dense layering (Haematocrit effect) in the pelvic cul-de-sac (Figure 2).
Intra-operatively, three litres of blood with clots were evacuated from the peritoneal cavity. Spleen was found shattered and free-floating with no ligamentous attachments. All other viscera were normal with no evidence of injury. She had an uneventful recovery in the postoperative period, was started on lifelong Penicillin, and was vaccinated after two weeks. She was able to restart her radiotherapy with compensation for the four-day gap in treatment. Histological evaluation was consistent with splenic rupture with no evidence of neoplasia (Figure 3).
Discussion
According to Orloff and Peskin1, splenic rupture may be regarded as ‘spontaneous’ only if there is no history of preceding trauma in an otherwise normal spleen not affected by intra and peri-splenic diseases or any other disease which can involve the spleen. The incidence of spontaneous rupture of a diseased spleen, even though rare, is higher than the spontaneous rupture of the normal spleen and is therefore regarded as pathologic rupture.
The exact mechanism of the rupture is still unknown; however, various possibilities have been described in the literature such as (i) Cellular hyperplasia and engorgement leads to increased intra-splenic tension (ii) Acute splenic congestion caused by reflex spasm of splenic vein (iii) Compression of the spleen by abdominal musculature during physiological activities such as coughing, sneezing, vomiting and sexual intercourse (iv) Rupture of the aneurysmal splenic artery (v) Portal venous congestion leading to chronic venous congestion (vi) Abnormally mobile spleen undergoes recurrent torsion causing splenic congestion.3
Spontaneous rupture of the spleen occurs most frequently in patients suffering from haematological malignancies. Haematological malignancies such as Non-Hodgkin’s Lymphoma, Acute Myeloid Leukaemia, Chronic Lymphocytic Leukaemia, and Acute Lymphoblastic Leukaemia are commonly associated with such patients.4 SSR has also been reported in patients with other haematological conditions, such as anticoagulants and anti-platelet drugs such as heparin, tpA, warfarin, and ticlopidine, and clopidogrel.4 A high index of suspicion is required to diagnose spontaneous splenic rupture (SSR) in such patients. Two signs which can give a clue to the presence of spontaneous splenic rupture are Kehr’s sign (referred pain to the left shoulder due to diaphragmatic irritation) and Balance’s sign (tender mass palpable in the left upper abdomen).5 One of the theoretical descriptions as the cause of trauma following coughing/vomiting is the violent contraction of the diaphragm, leading to traction on spleen via peritoneal reflection.
The radiological investigations are the mainstay for the diagnosis of SSR. The presence of elevated left hemidiaphragm on plain X-ray of the abdomen may suggest the diagnosis of SSR. Focused assessment sonography in trauma (FAST) using ultrasound is used frequently in an emergency for trauma patients to see the presence of fluid in the peritoneal cavity. FAST is regarded as the best non-invasive radiological modality for assessing the peritoneal cavity in unstable patients. It is an operator-dependent modality and cannot identify the source of bleed and type of fluid in the peritoneal cavity.3 CT scan is the gold standard to diagnose the source of bleed as well as the extent of injury to the organ and other associated injuries.6
Recently, there is a change in the management of patients with traumatic splenic rupture in favour of non-operative treatment. However, the treatment of SSR is not clear. It is challenging to select a subset of patients who can be managed non-operatively. Patients having refractory shock even after adequate resuscitation are the ideal candidates for emergency splenectomy. Non-operative management in splenic rupture is controversial. It is unknown whether the diseased spleen retains the ability to heal, whether it retains its normal immunologic functions and whether there are higher chances of re-bleed because the spleen is rendered more friable. Based on individual case reports and small case series, the literature suggests that the pathologic spleen can heal after non-traumatic rupture. In a study of 11 patients of SSR, Guth et al.7 observed that all patients made a full recovery with an average blood transfusion of less than 200ml.
Non-operative management may be considered in selected hemodynamically stable patients as re-bleeds are rare, and the complications of the operative procedure and immunologic functions of the spleen should not be overlooked. In certain patient’s splenic salvage have been reported in the form of splenorrhaphy or partial splenectomy.8 Finally, the hemodynamic status of the patient determines the need for operative or no-operative treatment. In this patient, hemodynamic instability culminated in exploratory laparotomy and splenectomy, although stable patients can be potentially managed conservatively.
Ethical considerations: Written and informed consent has been taken from the patient.
Conflict of interest statement: Authors declare that there are no competing interests.
References
- Orloff MJ, Peskin GW. Spontaneous rupture of the normal spleen: a surgical enigma. IntAbstrSurg 1958; 106:90.
- Wehbe E, Raffi S, Osborne D. Spontaneous splenic rupture precipitated by cough: A case report and a review of the literature. Scand J Gastroenterol 2008; 43:634-637.
- Renzulli P, Hostettler A, Schoepfer AM, Gloor B, Candinas D. Systematic review of atraumatic splenic rupture. Br J Surg 2009; 96:1114-1121.
- Albert S. Tu, Mai-Huong TT, Larson CR. Spontaneous splenic rupture: Report of 5 cases and a review of literature. American Society of Emergency radiology 1997; 4(6):415-418.
- Jeffery RB, Laing FC, Federle MP. Computed tomography of splenic trauma. Radiology 1981; 141:729.
- Guth AA, Pachter HL, Jacobowitz GR. Rupture of the pathologic spleen: is there a role for non operative therapy? J Trauma. 1996; 41:214-218.
- Peitzman AB, Heil B, Rivera L, Federle MB, Harbrecht BG, Clancy KD et al. Blunt splenic injury in adults: multi-institutional study of the Eastern Association for the surgery of Trauma. J Trauma 2000; 49:177-189.
- Crate MID, Payne CMJ. Is the diagnosis of spontaneous rupture of a normal spleen valid? J R Army Med Corps 1991;137: 50-1.