|
|
|
|
 |
|
| |
 |
|
|
Original Articles |
|
|
|
|
|
Keywords :
Barium, Gastric, Malignant, Mass. |
|
|
|
Uma Debi, Ishan Kumar, Vishal Sharma, Anindita Sinha, Lokesh Singh, Kaushal Kishor Prasad, Gita Bhagat Department of Gastroenterology, PGIMER, Chandigarh, Punjab, India.
Corresponding Author:
Dr Uma Debi Email: Debi_uma@yahoo.co.in
DOI:
http://dx.doi.org/10.7869/tg.517
Abstract
Background: Barium meal is a safe, non invasive, inexpensive and cost effective imaging technique. Most of the malignant gastric masses do present with non specific symptoms such as epigastric pain, dyspepsia, bloating, nausea, vomiting etc. It is imperative to be well acquainted of imaging features of malignant gastric masses on barium studies. Aim: Review the barium findings of various histopathologically proven malignant lesions of stomach and recognize the pattern of involvement. Material and Methods: The barium study films along with clinical and histopathological records were cumulated from the archives of radiology unit of the department of gastroenterology, PGIMER, Chandigarh between the period January 2009 to December 2014. 144 cases of gastric tumours were found, of which complete histopathological diagnosis was available in 69 cases, which were included in this study. Both double contrast and single contrast barium were included in this study. The radiographic findings were reviewed by two experienced gastrointestinal radiologists simultaneously to determine the morphology and location of these neoplasms. Results: Among 69 cases, carcinoma constituted the majority with 51 cases (73.9%) followed by malignant GIST in 10 cases(14.5%),8 cases(11.5%) were of NHL. Of the various findings, stricture and malignant ulcer were the most commonly obtained findings on barium study in carcinoma. Nodular fold thickening in lymphoma and large intra luminal polypoidal mass was common in cases of malignant GIST. Conclusion: Barium studies, particularly double contrast barium studies are accurate technique in diagnosing gastric carcinoma, with higher sensitivity and sensitivity. We further emphasize that barium study complement endoscopy in gastric malignancies ( by giving an idea to the endoscopist about the nature of the lesion) and should regain its position as one of the main diagnostic tools.
|
48uep6bbphidcol2|ID 48uep6bbphidvals|1901 48uep6bbph|2000F98CTab_Articles|Fulltext Introduction
With increasing availability of endoscopy and advanced cross sectional imaging modalities, the use of barium studies in diagnosis of GI abnormalities has been gradually displaced from the diagnostic algorithm1. However, being a safe, non invasive, inexpensive and cost effective imaging technique, upper gastrointestinal series is still utilized in considerable volume in the diagnostic workup of non specific upper GI symptoms such as epigastric pain, dyspepsia, bloating, nausea, vomiting etc2. There are many well acquainted imaging features of malignant gastric masses on barium studies but unfortunately it is become increasingly difficult, due to decline in gastrointestinal fluoroscopic techniques in their diagnostic evaluation. The purpose of this retrospective study is: (a) to review the barium findings of various histopathologically proven malignant lesions of stomach; (b) to assess various barium findings and recognize the pattern of involvement to suggest the type of neoplasm.
Material and Methods
This is a retrospective study where we reviewed digital barium study films along with clinical and histopatholo-gical records of all the cases having gastric lesions on upper GI studies were cumulated from the archives of radiology unit of the department of gastroenterology, PGIMER, Chandigarh. These cases were acquired between the period January 2009 to December 2014. This task was facilitated as the cases are separately archived in the department based on the location of the lesion, along with the available clinical record along with the endoscopy findings and histopathological diagnosis. When available, confirmatory hospital notes such as surgical details were also assessed. Cross sectional imaging study such as CECT performed in all the patients. 144 cases of gastric tumours were found. Endoscopy and biopsy was performed in all patients, of which complete histopathological diagnosis was available in 69 cases, which were included in this study. All the patients were not send for surgery, some of them underwent chemotherapy as well as radiotherapy. The age range was 17-69 years (mean age 43years). Male and female ratio was 3:1. Both double contrast and single contrast barium studies were included in this study. The choice of single and double barium studies depend on the indication of the patient. Double contrast barium studies performed for barium meal where as single contrast barium studies performed for barium meal follow through (BMFT). High density barium sulphate (BaSo4) – 200- 250% w/v used for double contrast where as low density BaSo4 – 40% w/v used for single contrast barium studies. The radiographic findings were reviewed by two experienced gastrointestinal radiologists simultaneously to determine the morphology and location of these neoplasms. The stomach was arbitrarily divided into GE junction (and distal esophagus), gastric cardia, fundus, greater curvature, lesser curvature, body, antropyloric region and duodenum. The cases were assessed according to involvement of various parts. Lesions were classified as segmental stricture (with or without features of gastric outlet obstruction), ulcerative lesions, one or multiple polypoidal/nodular filling defects, partial or complete linitis plastica, gastric fold abnormalities, large intra luminal mass. Malignant strictures were characterized by various degrees of segmental luminal narrowing with irregular margins with or without associated proximal gastric dilatation suggestive of gastric outlet obstruction. Small intraluminal polypoidal lesions were characterized by intra luminal protruded filling defects. These ranged from small subcentimetric lesions to large mass like filling defect which were separately classified. Gastric rugal fold abnormalities consisted of thickening, distortion, and nodularity of gastric rugal folds. We then correlated the findings with the available endoscopic, cross sectional imaging and histopathological findings. The findings were tabulated and analysed on the basis of specific location of involvement in relation of type of the underlying neoplasm.
Results
Of the 69 cases selected in our study, carcinoma constituted the majority with 51 cases (73.9%) followed by malignant gastrointestinal stromal tumor (GIST - most common mesenchymal tumour of gastrointestinal tract) in 10 cases(14.5%), and 8 cases (8.6%) were of lymphoma. Mucosal details and early gastric malignancies are well evaluated in double contrast barium studies. The distribution of the cases along with the involvement of various parts of stomach is discussed in table 1. In 51 cases of carcinoma, 18 cases were confined to cardia and fundus (Figure 2) 15 involved the body region along with greater and lesser curvature (Figure 3) whereas in 18 cases antropyloric region (Figure 4) was involved. In 10 cases of GIST, 2 cases were located in fundus region (Figure 12) and in 8 cases body (Figure 13), with greater and lesser curvatures were involved. These tumours ranged from 3 to 14 cm in maximum diameter. Amongst the 8 cases of lymphoma, 2 cases were diagnosed as maltoma which are located in body of stomach, 1 involved fundus (Figure 14) whereas rest of the 5 cases located in antropyloric region (Figure 15) along with concomitant involvement of duodenum (in 3 cases), body, greater and lesser curvatures in one cases each. All of these cases were identified histopathologically as Non Hodgkin’s Lymphoma. Figure 1 Bar diagram of barium meal shows the various radiological findings in the cases. Of the various findings, malignant ulcer and stricture (defined as narrowing of lumen of bowel) were the most commonly obtained findings on barium study in carcinoma. Nodular fold thickening was (seen as filling defect on barium meal) common findings in lymphoma and large intra luminal polypoidal mass was common in cases of malignant GIST. Table 1 shows distribution of all the 69 cases along with the various site of gastric involvement. Table 2 show various barium study findings according to site of involvement of 51 cases of gastric carcinoma. Areas of segmental narrowing / strictures and ulcers were the predominant findings. The strictures were more common in the ends of stomach (GE junction with cardia and antropyloric region whereas malignant ulcers were relatively evenly distributed. In one case infiltrative gastric carcinoma was presented as partial linitis plastica (defined as thickening and fibrous proliferation in the wall of the antropyloric region or body stomach caused by the infiltration of scirrhous carcinoma and ) (Figure 9) where as in another case distortion and destruction of mucosal folds were seen (Figure 11).
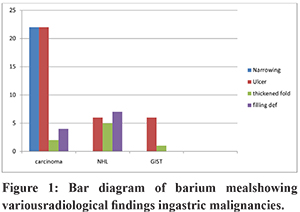
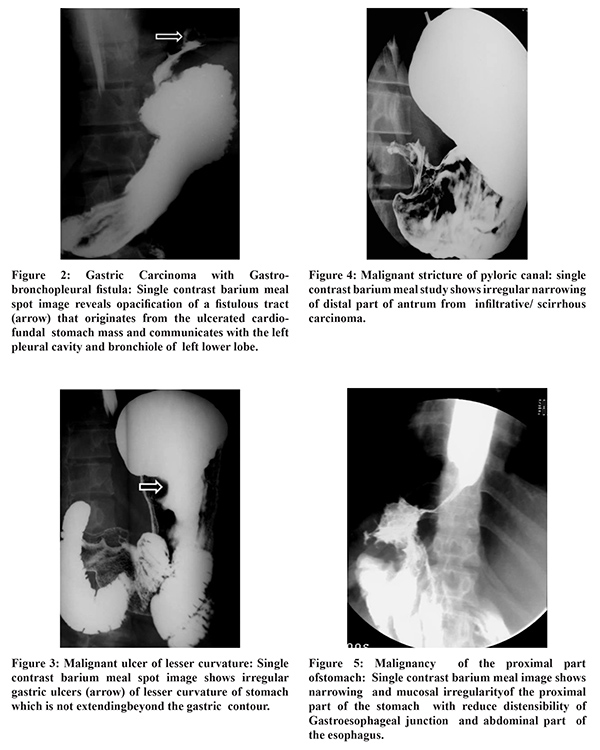
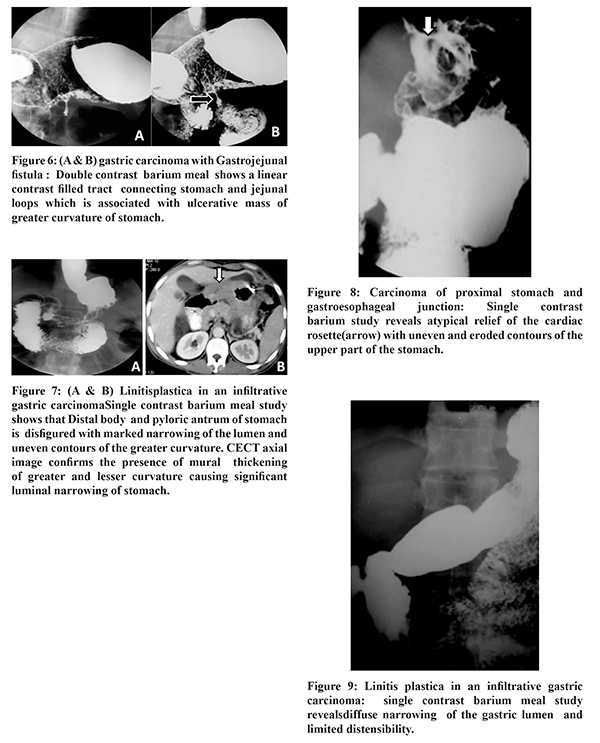
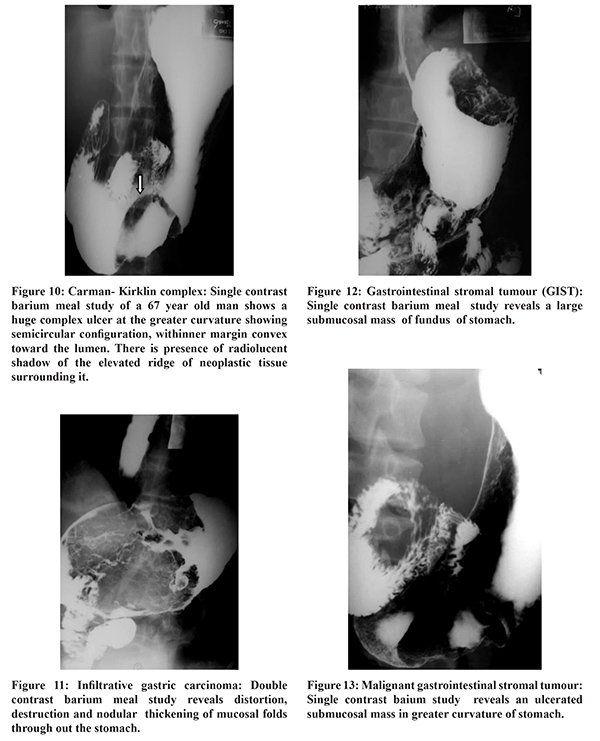
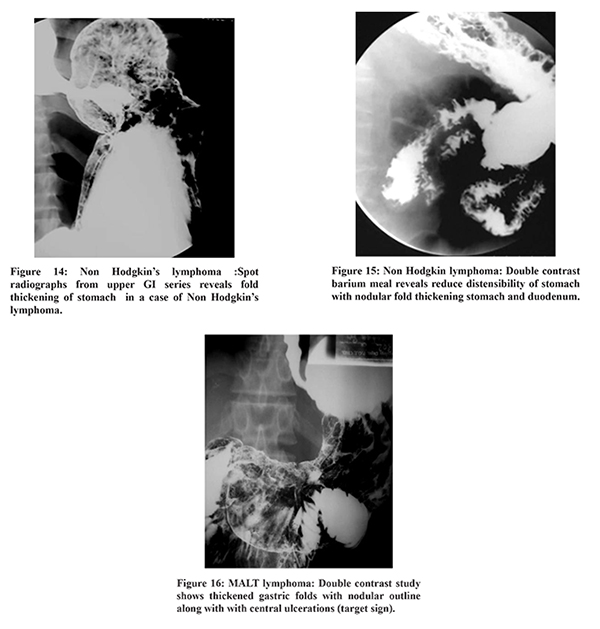
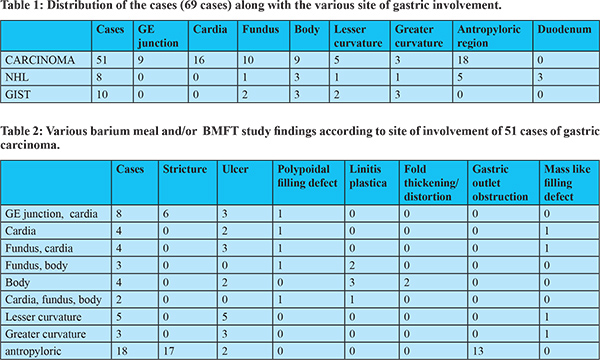
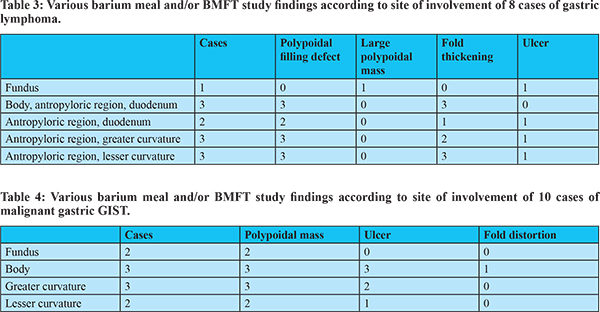
Table 3 discusses various barium study findings according to site of involvement of 8 cases of gastric lymphoma. Among them, 5 were seen involving antropyloric region, of which 3 has concomitant involvement of duodenum and 1 each were concomitantly involving greater and lesser curvatures respectively. Of the 3 cases involving duodenum and antropyloric region all showed polypoidal filling defect and 1 had presence of ulcer. Polypoidal filling defect was the most common finding (in 5 patient) and 1 patient had large polypoidal mass. Gastric fold thickening was present in 3 cases. Among the 8 cases of lymphoma, 2 cases were diagnosed as MALToma in our study were seen involving body of stomach. Both of these showed nodular fold thickening as well as nodularity of the normal thickness gastric folds. In addition one of these cases also showed multiple small nodular / polypoidal filling defects (Figure 16). Table 4 shows various barium study findings according to site of involvement of 10 cases of malignant gastric GIST. Most common finding was large polypoidal ulcerated mass. Out of 22 cases of strictures, all were present in carcinoma. None of the cases of lymphoma or GIST presented with stricture / segmental narrowing. Presence of concomitant malignant ulcer was seen in 3/22 cases, 2 of which was in GE junction and cardia (Figure 8) and 1 was located in antropyloric region (Figure 7). Of the remaining 19 cases of isolated stricture with irregular margins, 4 were seen involving GE junction (Figure 5) and cardia, 15 was present in antropyloric region. Of these 15 cases, 13 presented with clinical and radiological features of gastric outlet obstruction, seen as dilatation proximal to the lesion.
31 patients in our study had radiological picture of malignant ulcer. Of these, 14 had no other associated imaging abnormality and all were found to be carcinoma. 2 of these involved fundus and cardia (Figure 8), 3 were in cardia alone, 1 in fundus, 4 involved lesser curvature, 2 in greater curvature (Figure 10) and 2 in antropyloric region. Ulcerated large polypoidal mass was seen in 6 cases of malignant GIST, 1 case of lymphoma and 1 case of carcinoma. Both the cases of carcinoma and lymphoma was located at gastric cardia whereas, of 6 cases of malignant GIST, 3 cases were seen involving body, 2 involved greater curvature and 1 was in lesser curvature. Large polypoidal mass without ulcers showing smooth margin were present in 4 cases of malignant GIST, which were initially thought to represent benign submucosal mass on barium meal. Ulcer along with polypoidal filling defects were seen in 1 case of carcinoma involving GE junction and cardia, and 3 cases of lymphoma all of which involved antropyloric region, 1 with concomitant duodenal involvement and 1 with involvement of body along with antropyloric region. Multiple polypoidal filling defects without any other associated abnormality were present in 2 cases of lymphoma both involving antropyloric region and duodenum, and 3 cases of carcinoma with involvement of proximal stomach (body, fundus, cardia). 1 case of isolated multiple polypoidal filling defects were seen in MALToma involving body. 6 cases of partial or complete linitis plastica (Figure 9) were seen, all of them in carcinoma. 1 of these has associated fold thickening as well. All of these cases involved body of stomach with variable degree of involvement of other parts. 2 cases of carcinoma also presented with fistula. 1 of these was an ulcerated lesion in greater curvature with fistulous communication with jejunal loops (Figure 6). One of these was an ulcerated lesion in gastric cardia and fundus with fistulous communication with left pleural cavity and segmental bronchus of left lower lobe( Figure 2). Thickening of gastric folds were seen in 5 cases of lymphoma, 2 cases of carcinoma (Figure 11). The thickening was marked as nodular in three case of lymphoma and well marginated fold thickening was seen in 2 case of lymphoma.
Discussion Barium is radio opaque substance does not allow the passage of X-rays. As a result areas coated by Barium sulfate will appear white on an X-ray film. The contraindication of barium are colon obstruction, known or suspected, gastrointestinal tract perforation. There is no significant adverse affect of barium except for anaphylactoid reaction, appendicitis and fecal impaction. Study published by Vincent et al, showed that double contrast barium studies are accurate technique in diagnosing gastric carcinoma, sensitivity 99%3 where as we are able to diagnose all the cases of gastric malignancies on this retrospective study with sensitivity and specificity of 100%. Barium study still precedes upper GI endoscopy and cross sectional imaging in the evaluation of many cases of stomach neoplasms which may be clinically masked amongst these non specific clinical symptoms1 as in our study. Nishimata et al proved that double contrast barium studies in various position can detect all the cases of early gastric carcinoma with sensitivity and specificity of 100%4. Few authors showed that early gastric cancer detection rates are higher with endoscopy than with barium studies.5 Another study of Niigata, Japan, reported they the detection of gastric cancer by endoscopy screening was about 2.7 times higher than that by direct or indirect radiography screening7,6. Carcinoma is the most common malignant tumour of stomach, accounting for approximately 90-95% cases.The majority of cases in our study (74%) were carcinoma, with remaining cases of malignant GISTs and non Hodgkin lymphomas, all with varying radiological appearances and different anatomical seat of predilection. There has been increase in incidence of carcinoma in upper part of stomach in recent decades which has the worst prognosis. Early demonstration of the lesions in cardia and fundus may require double contrast study and various fluoroscopic manoeuvres7. Redistribution of gastric fundal air bubble or change in shape also has been suggested to be used in diagnosis of fundal masses with presence of gaseous tail inside the fundal mural thickening8. Antropyloric region is involved in 26% of the cases in gastric carcinomas. In the present study 18 patients (35%) had involvement of antropyloric region of which 17 presented with narrowing of the involved segment with irregular margins. 66% of the patients in the present study involving the body region showed radiological appearance of linitis plastica which is considered one of the most malignant forms of gastric carcinomas in which the tumour grows in the sub mucosal layer for a long time before eroding mucosal layer9. Given the high incidence of malignancy in the ulcers of greater curvature with upto 60% reported incidence (smith et al), ulcers in greater curvature with irregular contour should be further evaluated by endoscopy10. Stomach is the most common site of involvement of GISTs accounting for up to 60-70% cases11. Contrary to the concentric involvement of carcinomas, GISTs are commonly non obstructive in nature and more often revealed clinically by gastrointestinal bleed due to mucosal ulceration. On barium studies GISTs appear with features of large submucosal mass lesions with or without central ulceration12-15. In the present study, all the cases of the GISTs were seen as large submucosal lesion with 6 of them (60%) showing central ulceration. Primary lymphoma is responsible for 5-10 % of gastric malignancies. Stomach is the most common site of extra nodal lymphoma. In the present study among the 8 cases of lymphoma, 2 cases both had mucosal nodules revealed as filling defects on mucosal relief films as well as gastric fold thickening and diagnosed as low grade MALT lymphoma. Lymphoma, being a great mimicker of various benign and malignant diseases, can present with various imaging features ranging from fold thickening, ulcerated mass and filling defects however, obstruction is seldom a feature16-18. In the present study, polypoidal filling defects (5/8) was the most common finding along with gastric fold thickening (3/8) and 1 patient had large polypoidal mass. All but one cases involved the antropyloric region, of which majority showed transpyloric involvement of duodenum. Ulcerative lesions of carcinoma and lymphoma were difficult to distinguish many cases. Among all the patients, two were present with fistulous communication of stomach with jejunum and left broncho-pleural cavity with cardiofundal masses respectively. Both these cases were carcinoma on histopathological examination. Gastrobronchial fistula is a rare entity which has been described with gastric carcinoma. Gastrojejunal fistula has been described with gastric cancer as well as peptic ulcer disease21-23.
Conclusion
Barium studies, particularly double contrast barium studies are accurate technique in diagnosing gastric carcinoma, with higher sensitivity and sensitivity. Stricture, ulcer, linitis plastica, Gastric outlet obstruction commonly seen with gastric carcinoma where as thickened and distorted fold, Polypoidal filling defect are commonly associated with lymphoma and submucosal polypoidal mass lesion is commonly seen in GIST. We further emphasize that barium study complements endoscopy in gastric malignancies ( by giving an idea to the endoscopist about the nature of the lesion) and should regain its position as one of the main diagnostic tools .
References - Levine MS, Rubesin SE, Laufer I. Barium Studies in Modern Radiology: Do They Have a Role? Radiology. 2009; 250:18–22.
- Eisenberg RL. Gastrointestinal Radiology: A pattern approach. 3rd ed. Philadelphia: Lippincott; 1996.
- Low VH, Levine MS, Rubesin SE, Laufer I, Herlinger H. Diagnosis of gastric carcinoma: sensitivity of double-contrast barium studies. Am J Roentgenol.1994; 162:329–34.
- Portnoy LM. Radiologic Diagnosis of Gastric Cancer: A new Outlook. 1st ed. Heidelberg Germany: Springer Medizin Verlag; 2006.
- Choi KS, Jun JK, Park EC, et al. Performance of different gastric cancer screening methods in Korea: a population-based study. PLos One. 2012; 7: e50041.
- Tashiro A, Sano M, Kinameri K, Fujita K, Takeuchi Y. Comparing mass screening techniques for gastric cancer in Japan. World J Gastroenterol. 2006; 12:4873–74.
- Kumar RK, Raj SS, Shankar EM, Ganapathy E, Ebrahim AS, Farooq SM. Gastric carcinoma: A review on Epidemology, Current Surgical and Chemotheraputic options. Intech Open. 2013; 12: 271-93.
- Nishimata H, Maruyama M, Shimaoka S, Mishimata Y, Ohi H, Nihara T, et al. Early gastric carcinomas in the cardiac region: diagnosis with double contrast x-ray studies. Abdom Imaging. 2003; 28: 486-91.
- Wasch MG, Epstein BS. Roentgen visualization of tumours of the cardia. Am J Roentgenol. 1944; 51:564-71.
- Balthazar EJ, Rosenberg H, Davidian MM. Scirrhous carcinoma of the pyloric channel and distal gastric antrum. Am J Roentgenol. 1980; 134:669–73.
- Miettinen M, Lasota J. Gastrointestinal stromal tumor - definition, clinical, histological, Immunohistochemical, and molecular genetic features and differential diagnosis. Virchows Arch. 2001; 438:1–12.
- Levy AD, Remotti HE, Thompson WM, Sobin LH, Miettinen M. Gastrointestinal Stromal Tumors : radiologic features with pathologic correlation. RadioGraphics. 2003; 23:283–532.
- Nauert TC, Zornoza J, Ordonez N. Gastric leiomyosarcoma. Am J Roentgenol. 1982; 139:291–7.
- Sharp RM, Ansel HJ, Keel SB. Best cases from the AFIP: gastrointestinal stromal tumor. Radio- Graphics. 2001; 21:1557–60.
- Ghai S, Pattison J, Ghai S, O’Malley ME, Khalili K, Stephens M. Primary gastrointestinal lymphoma: spectrum of imaging findings with pathologic correlation. RadioGraphics. 2007; 27:1371–88.
- Engin G, Korman U. Gastrointestinal lymphoma: a spectrum of fluoroscopic and CT Findings. Diagn Interv Radiol. 2011; 17:255–65.
- An SK, Han JK, Kim YH, et al. Gastric mucosa- associated lymphoid tissue lymphoma: spectrum of findings at double-contrast gastrointestinal examination with pathologic correlation. RadioGraphics. 2001; 21:1491–1504.
- Gossios K, Katsimbri P, Tsianos E. CT features of gastric lymphoma. Eur Radiol. 2000; 10:425–30.
- Yoo CC, Levine MS, Furth EE, et al. Gastric mucosa- associated lymphoid tissue lymphoma: radiographic findings in six patients. Radiology. 1998; 208:239–43.
- Jha PK, Deiraniya AK, Roberts CSK, Das SR. Gastrobronchial fistula- a recent series. Interact Cardiovasc Thorac Surg .2003 ; 2: 6-8.
- Dias OM, Barbosa CCDL, Teixeira LR, Vargas FS. Gastropleural fistula from gastric perforation due to renal cell carcinoma after bevacizumab chemotherapy: a case report. Clinics. 2011; 66: 1495-98.
- Garrett KA, Rosati C. Gastro-Broncho-Pleural fistula after laproscopic gastric band placement. Obes Surg. 2009; 19: 941-3.
- Matsuoka M, Yoshida Y, Hayakawa K, Fukuchi S. Gastrojejunal fistula caused by gastric ulcer. J Gastroenterol. 1998; 33 : 267-71.
|
|
|
|
|
|