48uep6bbphidcol2|ID
48uep6bbphidvals|1910
48uep6bbph|2000F98CTab_Articles|Fulltext
First described nearly 500 years ago by Riverius in the 16th century, intestinal knotting remains an uncommon cause of mechanical bowel obstruction.1 Rotation of a segment of the intestine, along with its mesentery, leads to closed-loop obstruction. Compromise of the vascularity results in the rapid onset of ischemia of the affected segment.
Various types of intestinal knots have been described - ileo-sigmoid, appendico-ileal, ileo-caecal, ceco-sigmoid, around a Meckel’s diverticulum,and ileo-ileal.1-3 Ileo-sigmoid knotting (ISK) is by far the most frequently encountered, in which loops of ileum and distal jejunum twist around thebase of a narrow sigmoid colon. Factors associated with ISK and intestinal knotting, in general, are a freely mobile small intestine, redundant sigmoid colon, long and narrow mesocolon, high fiber diet, and ingestion of a single daily meal.1-3 Unfortunately, there is a paucity of literature on ileo-ileal knotting, and only 9 cases have been reported in the literature, to our knowledge.2,4
We report another such case of this rare cause of intestinal obstruction that occurred in a patient who underwent laparoscopic cholecystectomy at our Institute, and review relevant literature.
Case Report
A 65 year old lady underwent elective laparoscopic cholecystectomy (LC) at our hospital for symptomatic gallstones. A standard four-port LC was performed under general anesthesia with the first (infra-umbilical) port being placed by an open technique using the umbilical pillar. Laparoscopic examination of the abdomen was normal, and then cholecystectomy was performed, with gallbladder removal via the epigastric port, without complications and discharged the next day. On follow up visit to our outpatient clinic, she complained of occasional abdominal pain. Abdominal examination was normal, and she was advised analgesics on as needed basis.
On the 15th post-operative day, she presented to the emergency in the evening with complaints of abdominal distension and vomiting; there was no fever, tachycardia, or abdominal rebound tenderness, but there was a fullness in the right lower abdomen. She was managed conservatively with suspicion of post LC bile leak, ductal injury, or acute pancreatitis. Ultrasound of the abdomen did not reveal any collection and we proceeded with a contrast-enhanced computerized tomography (CECT) scan of the abdomen the next day, which revealed a grossly patent ductal system and a healthy pancreas. There was mesenteric stranding along with dilatation of the small bowel up to a transition zone beyond which dye could not pass, but no mass or intra-abdominal collections were seen. The patient developed fever, tachycardia, and abdominal rebound the next day, and was taken up for emergency surgery at the earliest.
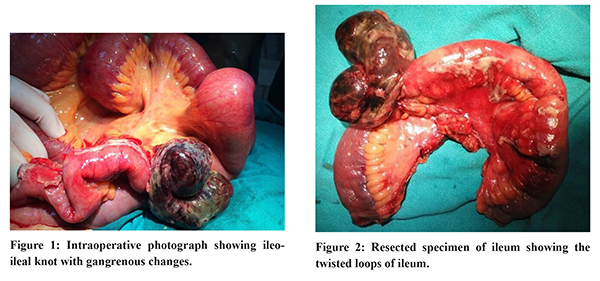
Laparotomy was performed by a midline incision, and minimal dirty, serosanguinous fluid was seen, along with dilatated jejunal and ileal loops. On further exploration, a firm lump was felt in the distal ileum, about two feet proximal to the ileocecal junction (Figure 1). Upon delivery through the midline, a loop of the ileum was found to have twisted upon itself, and its mesentery, to cause strangulation obstruction. A part of this loop was already blackened and gangrenous with impending perforation. The ileum bearing this ‘knot’ as well as unhealthy bowel adjacent to it were resected (Figure 2). Exploration of the abdomen did not reveal any other pathology, and we were also able to visualize the common bile duct and the site of clips on the cystic duct during the previous LC. An ileostomy (as well as mucus fistula) was fashioned in the right lower abdomen, and the abdomen closed.
The patient remained well in the post-operative period and, at last follow up, was scheduled for the elective restoration of bowel continuity. Histopathology of the resected specimen revealed oedematous mucosa and submucosa with transmural infarction, congested blood vessels along with acute inflammatory cellular infiltrate.
Discussion
LC is associated with its particular group of complications, but the present case of ileal knotting occurring post-LC is probably coincidental rather than as a consequence of LC. The etiology of ileo-ileal knotting is poorly understood, and differential mobility of small bowel loops and changes in their relative intra-abdominal positions after meals (as hypothesized in ISK) may contribute.1-5 The presence of adhesions, around which loops of small bowel might twist, has also been hypothesized5 possibly, altered gut mobility6 after LC in our patient may have in some way contributed to the knotting of the ileum upon itself, but a definite etiology remains obscure.
As there are no pathognomic etiological, clinical or radiological features, ileo-ileal knotting is usually not diagnosed pre-operatively;1,2,5 these patients present with symptoms and signs of intestinal obstruction, and as is the case when strangulation occurs, progress rapidly towards septicemia and multi-organ failure due to intestinal occlusion, ischemia, and gangrene.1-3,5 The condition is often diagnosed intra-operatively, once the knot is visualized. If the bowel is viable and strangulation has not yet supervened, untying the knot is recommended1-3,5 since recurrence is uncommon.1 However, this carries a risk of perforation, especially if multiple attempts are made.1-3,5 If the bowel unviable, as in our patient, en bloc resection of the segment after controlled decompression of its contents followed by exteriorization or anastomosis, based on the surgeon’s experience is preferred.1-5
References
- Uday S, Venkata PKC, Bhargav P, Kumar S. Ileo-ileal knot causing small bowel gangrene: an unusual presentation. Int J Case Rep Imag 2012;3:28-30. doi: 10.5348/ ijcri-2012-05-121-CR-6
- Taniguchi K, Iida R, Watanabe T, Nitta M, Tomioka M, Uchiyama K, Takasu A. Ileo-ileal knot: a rare case of acute strangulated intestinal obstruction. Nagoya J Med Sci. 2017;79:109-113. doi: 10.18999/nagjms.79.1.109
- Abebe E, Asmare B, Addise A. Ileo-ileal knotting as an uncommon cause of acute intestinal obstruction. J Surg Case Rep. 2015; 8: 1 - 2.doi: 10.1093/jscr/rjv102
- Kalachelvan L, Perumal SU, Ross K, Subramanian B. Ileo-Ileal Knot Causing Intestinal Obstruction – A Case Report. OSR-JDMS 2016; 15: 26 – 9. DOI: 10.9790/0853-150732629
- Gopivallabh MM, Jaganmaya K, Hanumanthaiah KS, Babannavar P, Crithic V. Ileoileal Knot as a Content of Obstructed Hernia: What Are the Odds? Iran J Med Sci. 2016; 41:238–240
- Madacsy L, Dubravcsik Z, Szepes A (2015) Postcholecystectomy Syndrome: From Pathophysiology to Differential Diagnosis - A Critical Review. PancreatDisordTher 5: 162. doi:10.4172/2165-7092.1000162