48uep6bbphidcol2|ID
48uep6bbphidvals|1903
48uep6bbph|2000F98CTab_Articles|Fulltext
Endoscopic ultrasound (EUS) guided transaortic fine needle aspiration (FNA) is well reported in the literature. We present a case of prospective liver transplant recipient in whom the PET-CT scan showed intra-abdominal lymphadenopathy, and EUS suggested pathological para-aortic lymph nodes with the only access through both aorta and inferior vena cava. We performed a trans-caval plus trans-aortic FNA with the aspirate cytopathology positive for malignant cells; thus, a futile liver transplantation surgery could be avoided.
Case Report
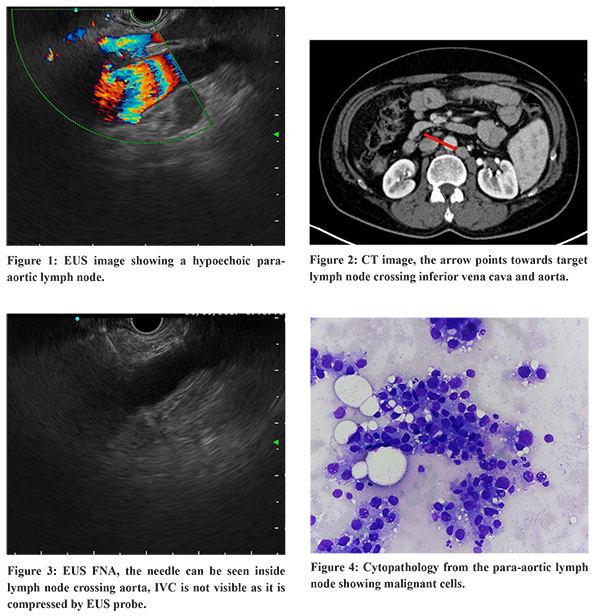
A 52-year-old male was evaluated for liver transplantation for hepatitis B related cirrhosis and hepatocellular carcinoma (HCC). His Childs’ score was 8, and model for end-stage liver disease (MELD) score was 13. His platelet count was 1.7x103/cmm, and INR was 1.24. A PET-CT performed routinely in cases of HCC, to rule put extra-hepatic disease, showed FDG avid primary lesion in the liver and mildly FDG avid small (< 1 cm at short axis) abdominal lymph nodes at portocaval and para-aortic locations. EUS FNA of the portocaval node was suggestive of reactive change; however, the morphologic features of the para-aortic lymph node on EUS were suggestive of pathologic change (round to oval shape, hypoechoic, defined borders, Figure 1). The access to this para-aortic lymph node was only through both the inferior vena cava and aorta (Figure 2). The case was considered for image-guided percutaneous FNA or surgery; however, a decision for EUS guided trans-caval plus transaortic FNA was made, given the complicated interventional radiological access and high risk of post-surgery decompensation/mortality in view cirrhosis. EUS FNA sample was obtained with a 25G needle (Figure 3) without fanning to avoid the shearing of the vascular wall, and an on-site cytopathologist was present to minimize the number of passes. The first pass was positive for malignant cells (Figure 4). The patient was monitored for bleed after FNA; EUS did not show any hematoma. The patient remained asymptomatic post-procedure. Given the disseminated disease, futile liver transplantation could be avoided.
Discussion
EUS guided transaortic FNA, and CT guided transcaval biopsies have been reported,1-3 without significant complication. EUS guided trans inferior vena cava FNA has been reported from our center.4 The current case report highlights two critical issues: EUS increases the reach of FNA from difficult locations, and that suspicious lymph nodes should be sampled before liver transplantation. We previously reported our experience of routine lymph node FNA in patients with hepatocellular carcinoma before liver transplantation in which out of 50 patients who underwent EUS guided FNA, metastatic lymphadenopathy was present in 15 (30%) cases.5 This is the first report, to the best of our knowledge, describing a transcaval plus transaortic approach for EUS FNA in cases of HCC.
References
- von Bartheld MB, Rabe KF, Annema JT. Transaortic EUS-guided FNA in the diagnosis of lung tumors and lymph nodes. Gastrointest Endosc. 2009 ;69:345-9
- Sofocleous CT, Schubert J, Brown KT, Brody LA, Covey AM, Getrajdman GI. CT-guided transvenous or transcaval needle biopsy of pancreatic and peripancreatic lesions. J Vasc Interv Radiol 2004;15:1099-104
- Somani P, Sharma M. Transaortic EUS Guided FNA in the Diagnosis of Lung Cancers and Mediastinal Lymph Nodes. Gastrointest Endosc 2017; 85(5) Supplement: Page AB145
- Choudhary NS, Bansal RK, Puri R, Guleria M, Sud R. Endoscopic ultrasound-guided fine-needle aspiration of an aortocaval lymph node by the transcaval approach. J Dig Endosc 2016;7: 58-159
- Choudhary NS, Puri R, Saigal S, Bhangui P, Saraf N, Shah V et al. Impact of endoscopic ultrasound-guided fine-needle aspiration in prospective liver transplant recipients with hepatocellular carcinoma and lymphadenopathy. Ind J Gastroenterol. 2016;35:465-468