48uep6bbphidcol2|ID
48uep6bbphidvals|1890
48uep6bbph|2000F98CTab_Articles|Fulltext
Thoracic aorta intramural thrombosis accounts for 0.9% of all etiologies of peripheral arterial thrombosis1. The frequent origins are intracardiac, intraaneurysmal, atherosclerotic lesions, trauma, malignancies and coagulation disorders2. The current use of echocardiography and computed tomography has facilitated in early diagnosis of aortic thrombosis as a cause for peripheral thromboembolic episode3. The purpose of the case report is to review the diagnostic capability of endoscopic ultrasound (EUS) beyond the routine evaluation of gastrointestinal organs.
Case Report
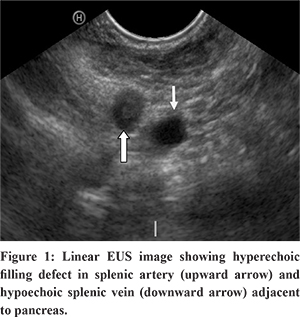
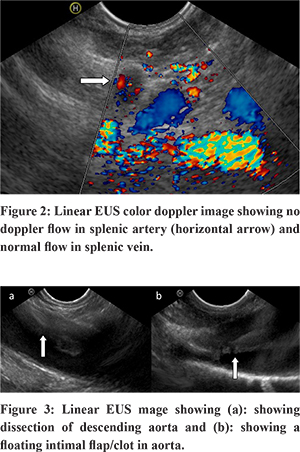
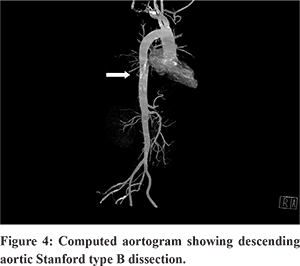
A 48 year old male, presented to the emergency department with severe chest and abdominal pain for 3 days duration. He denied any history of shortness of breath or palpitations. He was a known hypertensive on treatment for 8 months. He had no habits. Physical examination was unremarkable. He was evaluated at a local hospital and was prescribed an anti-inflammatory and anti spasmodic for pain but he reported no improvement. Ultrasound abdomen revealed a hypo echoic spleen, probably an abscess or infarct and was referred for evaluation of the same. Laboratory test results were all within normal limits including common blood cell counts, liver chemistries, renal parameters and serum lipase. Contrast enhanced computed tomogram of the abdomen and pelvis showed splenic infarct secondary to splenic artery thrombosis and segmental renal infarcts due to renal artery thrombosis.Transthoracic echocardiography (TTE) showed neither valvular nor intra cavitary anomalies. Ventricular ejection fraction was preserved. He was referred for Endoscopic Ultrasound (EUS) evaluation of splenic artery thrombus and for ruling out any pancreatic pathology.With a Pentax EG-3870UTK endoscope coupled to a Hitachi HI Vision Avius estiva console (ultrasound beam frequency at 7.5 MHz), endoscopic ultrasound was performed without complications. EUS showed a splenic artery thrombosis and splenic infarct (Figure 1). On colour doppler evaluation, flow was noted in splenic vein and no flow in splenic artery (Figure 2). The surrounding pancreatic parenchyma, aorta with celiac take off was normal. The thrombus in the splenic artery was noted from the celiac bifurcation. The outer border of descending aorta abuts against the left lung and makes a mirror image artifact because of the reflection of sound waves from the lung. Mediastinal examination showed dissection in descending aorta with a linear intraluminal floating clot which was traced both by pushing along the posterior wall of the esophagus from the arch downwards or by withdrawing from celiac take off (Figure 3). A diagnosis of aortic dissection with adherent clot and a thromboembolic episode to spleen was made. Computed aortogram (Figure 4) confirmed the findings, classified it as Stanford type B and was started on anticoagulation and beta blockers. He was asymptomatic at 6 months of follow up.
Discussion
Trans esophageal echocardiogram is most commonly performed to evaluate for a potential cardiac source of embolus4 and to evaluate for suspected acute aortic pathology (i.e., dissection)5. In our case, the etiological investigation for aortic thrombus found no hematological abnormalities and the only cardiovascular risk factors was hypertension. In the study of Turley6, 83% of aortic thrombosis treated with anticoagulation, had complete resolution of the thrombus with one amputation as a complication was reported.
With increasing use of EUS as a diagnostic and therapeutic technique, it can provide an unique access to vascular structures in the mediastinum and abdomen. EUS probes provide high quality 2D resolution, color doppler, and pulsed doppler images. Aortic floating thrombus is a rare, life-threatening disease with predisposing abnormal coagulation function, aortic disease, and history of aortic stent implantation. Echoendoscopic evaluation of proximal aorta can confirm the diagnosis in distal embolic phenomenon, endoscopic ultrasonographers to extend the horizons of EUS beyond the limits of current practice.
References
- Tsilimparis N, Hanack U, Pisimisis G, Yousefi S, Wintzer C, Rückert RI. Thrombus in the non- aneurysmal, non atherosclerotic descending thoracic aorta - An unusual source of arterial embolism. Eur J VascEndovasc Surg. 2011;41:450–7.
- Yves GhislainAbissegue, Youssef Lyazidi, Hassan Chtata, Tarik Bakkali, and Mustapha TaberkantAcute systemic embolism due to an idiopathic floating thrombus of the thoracic aorta: success of medical management: a case report. BMC Res Notes. 2015; 8: 181.
- Blangetti I, Fenoglio L, Avallato C, Bertora M, Novali C, Peinetti F, et al. Transesophagealecocardiography: the correct intraoperative Way to detect the source of peripheral embolism in an emergency. Ann Vasc Surg. 2013;27(8):e13–1185.
- Oh JK, Seward JB, Tajik AJ. Transesophageal and Intracardiac Echocardiogrphy. In: The Echo Manual, 3rd edition, Lippincott Williams & Wilkins. 2007. p.29-30.
- American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardiography, American Heart Association, et al. J Am Coll Cardiol. 2011; 57:1126.
- Turley SR, Unger J, Cox MW, Lawson J, McCann RL, Shortell CK. Atypical aortic thrombus: should nonoperative management Be first line? Ann Vasc Surg. 2014;28(7):1610–7.