48uep6bbphidcol2|ID
48uep6bbphidvals|1860
48uep6bbph|2000F98CTab_Articles|Fulltext
Testicular cancer is a rare malignancy among men however it is the most common malignancy among young in the west. Choriocarcinoma accounts for 1% of the germ cell tumour of testes and has the most aggressive behaviour with majority presenting with metastatic disease.1 Here we present a case of a young male who presented with massive upper gastrointestinal bleed and was found to have a friable, polypoidal lesion in the jejunum that was actively oozing and patient had very high values of beta HCG along with a bulky right testis which responded to combination chemotherapy.
Case Report
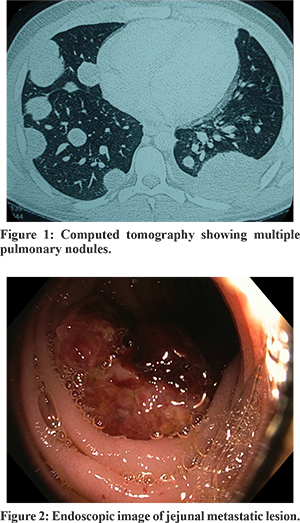
A 28 year old male presented with three weeks history of easy fatigability and palpitations. Before coming to our centre his examination chart outside showed rate of pulse 110/min, blood pressure 110/60 mmHg, respiratory rate of 18/min. His systemic examination was unremarkable. His investigations showed haemoglobin 4.0gm %, TLC 11600/dl, platelet 2.55 lacs/dl. The liver function test revealed raised transaminases with hypoalbuminemia (bilirubin 1.6 mg/dl, AST/ALT 44/51IU/L, ALP 63 IU/L, total protein 3.25, albumin 2.7gm/dl). The renal function tests were normal with blood urea 24 mg/dl, creatinine 0.72 mg/dl, serum sodium 130 mg/dl, potassium 3.5 mg/dl. His esophagogastroduodenoscopy and colonoscopy were done elsewhere which were normal. With this he was referred to our centre for capsule endoscopy. At presentation, he had tachycardia with pulse 120/min and had pallor. Rest other general systemic parameters were normal. His haemoglobin was still low 6.5gm% despite receiving four units of blood transfusion. His chest X-ray showed bilateral cannon ball opacities confirmed on computed tomography (Figure 1). On further questioning patients gave history of sense of heaviness in the right testis occasionally so an ultrasound of the testes was ordered which showed right bulky heterogenous testis measuring 5.25 cm. The levels of beta HCG and alpha feto protein were ordered which wereelevated (beta HCG 1,21,374 IU/L and alpha fetoprotein 19.4 ng/dl) and LDH was also elevated at 1020 IU/L. We did a push enteroscopy and a friable, polypoidal growth partially occluding the lumen with slight ooze was noted in the proximal jejunum (figure 2). Therefore a diagnosis of metastatic choriocarcinoma presenting as bleeding from jejunal metastasis was made and the patient received chemotherapy with combination of bleomycin, etoposide and cisplatin. The patient was discharged after first session with cessation of bleeding and stable haemoglobin at 10gram/dL.
Discussion
Choriocarcinoma is an aggressive germ cell tumours with early metastatic presentation from early vascular invasion due to the predominant trophoblastic component of the tumour. Choriocarcinoma syndrome is one the dreaded manifestation of metastatic choriocarcinoma where the patients present with bleeding manifestation from the metastatic tumour deposits.2 It can occur after the initiation of chemotherapy due to tumour lysis syndrome or spontaneously from metastatic tumour deposits which invade the small blood vessels as was seen in our patient.3 The prognosis in this syndrome is very poor especially in those with very high beta HCG levels above 50,000 IU/L.4 It’s a life threatening condition especially when the bleeding occurs from pulmonary or liver metastasis as patient can die of exsanguination even with successful chemotherapy. So, early and prompt intervention with multimodality approach is needed with management in an intensive care unit with prompt initiation of the standard chemotherapy of BEP protocol (Bleomycin, eotposide and cisplatin) even without the histology reportand surgical intervention when it is appropriate.5We started chemotherapy for our patient without waiting for the histology as the beta HCG was > 50,000 IU/L and as a result the patient was stabilized and is now doing well under follow up.
References
- Schmoll HJ, Souchon R, Krege S, Albers P, Beyer J, KollmannsbergerC,et al ; European Germ Cell Cancer Consensus Group.. European consensus on diagnosis and treatment of germ cell cancer: a report of the European Germ Cell Cancer Consensus Group (EGCCCG). Ann Oncol 2004;15:1377-99.3.
- Kawai K, Takaoka E, Naoi M, Mori K, Minami M, Shimazui T, Akaza H. A case of metastatic testicular cancer complicated by tumour lysis syndrome and choriocarcinoma syndrome. Jpn J Clin Oncol 2006;36:665-7.6.
- Motzer RJ, Bosl GJ. Hemorrhage: a complication of metastatic testicular choriocarcinoma. Urology. 1987;30:119-22.7.
- Durieu I, Berger N, Loire R, Gamondes JP, Guillaud PH, Cordier JF. Contralateral haemorrhagic pulmonary metastases (“choriocarcinoma syndrome”) after pneumonectomy for primary pulmonary choriocarcinoma. Thorax. 1994;49:523-48.
- Voskuil JH, Slee PH, Wagenaar SS. The choriocarcinoma syndrome: an emergency. Neth J Med. 1995;46:232-5.