48uep6bbphidcol2|ID
48uep6bbphidvals|1868
48uep6bbph|2000F98CTab_Articles|Fulltext
Gastric adenocarcinoma with yolk sac differentiation are rare tumours. They are usually AFP secretors and presents with high AFP levels. Also the neoplastic cells on histology show presence of PAS positive hyaline globules which stains with AFP IHC. In presence of liver metastasis distinction from primary hepatocellular carcinoma is crucial. Most of these cases have a dismal prognosis with early metastasis. Presence of fungal coinfection may accelerate the disease progression as was seen in our case.
Case Report
We report a case of a 76-year-old male who presented with syncope. He was evaluated at an outside hospital where he was found of have severe anaemia with a haemoglobin of 4.4 (13-17 g/dl). He received 2 units of packed RBC’sthere. Stool for occult blood was positive. Laboratory examination revealed deranged liver enzyme with OT/ PT of 72/24 (15-37 U/L) (30-65 U/L), alkaline phosphatase of 722 U/L(50-136/L), and GGT of 348 U/L(5-85). CT head done was normal. USG abdomen showed a large liver space occupying lesion. Anti HCV,HbsAg and HIV were non reactive. Alpha feto protein was 11,414 ng/ml (0.2-9 ng/ml).
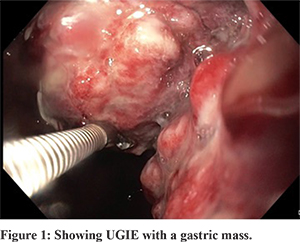
Upper gastrointestinal endoscopy showed a large growth starting from GE junction and extending along the lesser curvature occupying almost 30% of the circumference and extending up to the corpus antral junction, highly friable suggestive of gastric cancer (Figure 1).
CECT showed a stomach mass with? Locoregional spread. Liver mass? secondary to portal vein thrombosis. Histology from the biopsy tissue show an adenocarcinoma with reticular areas composed of cells showing prominent PAS positive hyaline globules. Surface show numerous entangled fungal hyphae. IHC performed showed the tumor cells were positive for CK7, CDX2 and negative for HepPar 1, Arginase and CK 20. The hyaline globules were positive for AFP (Figure 2). FNAC from the liver mass showed a metastatic adenocarcinoma with presence of similar PAS positive globules. Cell block prepared showed the globules are AFP positive and the neoplastic cells are positive for CK7, CDX 2 and negative for CK 20 and HepPar 1 and Arginase (Figure 3).
So a final diagnosis of Gastric Adenocarcinoma with yolk sac differentiation, superadded fungal infection and liver metastasis was rendered.
Patient performance status was poor so chemotherapy was initially not given. Patient condition deteriorated thereafter and he became bed ridden. He died within one month after diagnosis.
Discussion
Gastric mucosal adenocarcinoma with yolk sac differentiation was first described by Garcia etal in 1985 in a 65-year-old male. There are two theories for the possible origin of this differentiation -forward differentiation of neoplastic germ cells in the gonads and retro-differentiation (opisthoplasia) of neoplastic mucosal epithelial cells in the stomach. Ooi etal on a study on 5 cases postulated that gastric adenocarcinoma with yolk sac differentiation are not always derived from hepatoid differentiation of the foregut. These tumours are to be categorized into medullary tumor with gastrointestinal tract-specific AFP.1
Motoyama etal proposed a classification for AFP producing gastric carcinoma based on a study on 9 cases. They proposed three subtypes of these tumoursas: (i) hepatoid type; (ii) yolk sac tumor-like type; and (iii) fetal gastrointestinal type. Hepatoid type are derived from liver cell metaplasia and yolk cell type by yolk sac cell metaplasia of common poorly differentiated medullary adenocarcinoma, respectively. The fetal gastrointestinal type seemed to be a result of the imitation of fetal gastrointestinal epithelium by common tubular adenocarcinoma. The hepatoid type was the most common and highly malignant typeof AFP-producing gastric carcinoma.
AFP producing adenocarcinomas have also been described in other organs like pancreas, gastric stump etc
Histology of these tumours show mixture of areas of adenocarcinoma with reticular pattern composed of cells showing presence of PAS-D positive hyaline globules which are AFP positive. Rarely cases can show dual yolk sac and choriocarcinomatous differentiation.2
Prognosis of these cases is dismal with most patients presenting with early liver or lymph node metastasis.Chang etal has described 3 cases of AFP producing early gastric carcinoma presenting with early liver metastasis. Age of patients ranged from 59 -65 years with a male: female ratio of 2:1. AFP in these patients were 1, 146 and 800 ng/ml respectively. Surgery was done in all and all three patients died within 2 years of surgery.3
Gastric adenocarcinoma with yolk sac differentiation are very rare tumours with very few cases reported in English literature.4,5 Cases presenting with solitary liver metastasis are still rarer with only 5 case reported. These cases pose a major diagnostic challenge. Differentiating them from synchronous hepatocellular carcinoma is a major challenge as AFP levels are also raised in both. The immunohistochemical panel for primary hepatocellular markers and gastric markers performed on cell block/ biopsy will guide in reaching to correct diagnosis. Gastric carcinomas with yolk sac differentiation are CDX2, CK7, SALL4 and AFP positive whereas primary hepatocellular carcinoma are CDX2 negative and positive for HepPar 1and Arginase.
References
- Ooi A, Nakanishi I, Sakamoto N, Tsukada Y, Takahashi Y, Minamoto T, Mai M. Alpha-fetoprotein (AFP)-producing gastric carcinoma. Is it hepatoid differentiation?Cancer. 1990 Apr 15;65(8):1741-7.
- N. Satake, M. Chikakiyo, T. Yagi, Y. Suzuki, and T. Hirose, “Gastric cancer with choriocarcinoma and yolk sac tumor components: case report,” Pathology International 2011; 61 (3):156–160
- Morinaga S, Takahashi Y. Primary hepatocellular carcinoma and hepatoid adenocarcinoma of the stomach with liver metastasis: an unusual association.Jpn J Clin Oncol. 1996 ;26(4):258-63.
- Tsurumachi T, Yamamoto H, Watanabe K, Honda I, Watanabe S, Yamada S, Jingu K, Satomi D, Fujita M. Resection of liver metastasis from alpha-fetoprotein-producing early gastric cancer: report of a case. Surg Today. 1997;27(6):563-6.
- DeLorimier A, Park F, Aranha GV, Reyes C.Hepatoid carcinoma of the stomach. Cancer. 1993 Jan 15;71(2):293-6.