48uep6bbphidcol2|ID
48uep6bbphidvals|1816
48uep6bbph|2000F98CTab_Articles|Fulltext
Pancreatic fluid collections (PFCs) are an important local complication of acute pancreatitis that are associated with significant morbidity.1 Pseudocyst and walled off pancreatic necrosis (WOPN) are the delayed consequences of these collections. The pancreatic pseudocyst is defined as an encapsulated collection containing minimal solid material, whereas WOPN is an encapsulated collection of solid necrotic material with varying amount of liquid content.1 This distinction is important as patients with WOPN usually require more aggressive endoscopic drainage, in contrast to simple transmural drainage which may be adequate for treatment of pseudocysts.2-5 The aggressive endoscopic drainage involves use of multiple plastic stents, fully covered self-expanding metallic stents (FC-SEMS) or direct endoscopic necrosectomy (DEN). The SEMS offer theoretical advantages, including a larger lumen diameter that allows easy DEN as well as need of fewer procedures. Stent migration is a well known complication of FC-SEMS and it is usually outward migration. In this case report, we report an inward migration of SEMS that was successfully retrieved endoscopically.
Case Report
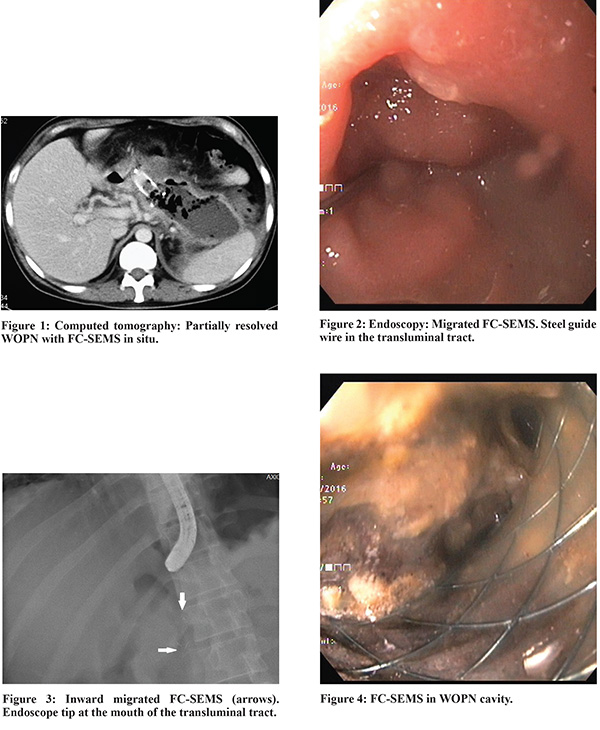
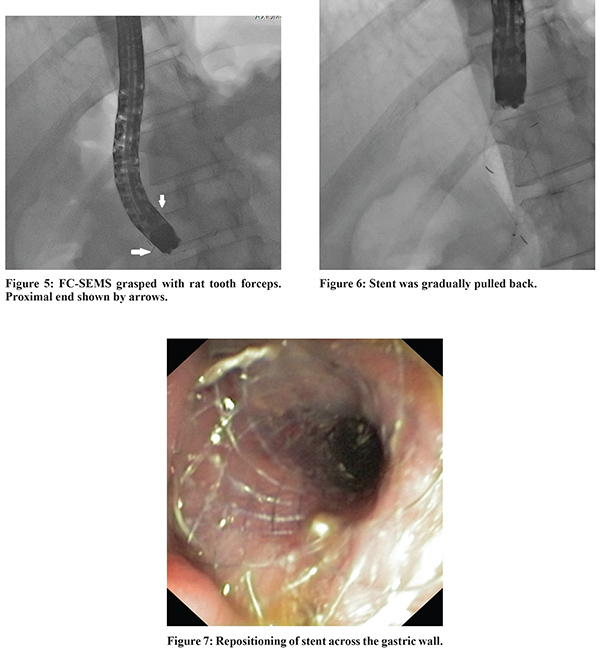
A 34 year old male with a large 18 cm walled off pancreatic necrosis consequent to alcohol related acute necrotizing pancreatitis presented with abdominal pain and fever. He underwent endoscopic ultrasound (EUS) guided transmural drainage using a fully covered self-expanding metallic stent (FC-SEMS) with wide flared ends (NAGI stent, Taewoong Medical Co., Ltd., Seoul, Korea). The WOPN decreased in size (Figure 1) but pain and fever persisted. Therefore, the patient was taken up for direct endoscopic necrosectomy. On endoscopy, the stent was not visualized (Figure 2) and fluoroscopy revealed migration of SEMS into WOPN cavity (Figure 3). The endoscope was pushed into the cavity over steel guide wire and stent could be seen inside the necrotic cavity (Figure 4). The retrieval string of the stent was identified and grasped with rat tooth forceps (Figure 5). The stent was gradually pulled back (Figure 6) and repositioned across the stomach (Figure 7) establishing transluminal drainage. Thereafter, endoscopic necrosectomy was done and patient had marked resolution of symptoms after 3 session of necrosectomy. The SEMS was removed 6 weeks later and replaced with two 10 Fr double pigtail plastic stents. Thereafter, patient was discharged and is asymptomatic on follow up.
Discussion
Endoscopic transluminal drainage of WOPN involves using more aggressive techniques such as placement of multiple stents, aggressive irrigation using nasocystic catheter, and direct debridement of necrotic tissue.1-5 FC-SEMS provide a larger diameter for drainage and also decrease risk of perforation and bleeding because of minimal dilation and sealing of the fistula tract.6 The FC-SEMS have higher risk of migration but large and acute angled flare ends decrease risk of migration. Migration has been occasionally reported but mostly it is outward and inward migration is very rare, in which case endoscopic recovery is possible.6
References
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis-2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013;62:102–11.
- Rana SS, Bhasin DK, Rao C,Gupta R, Singh K. Non-fluoroscopic endoscopic ultrasound-guided transmural drainage of symptomatic non-bulging walled-off pancreatic necrosis. Dig Endosc. 2013;25:47–52.
- Gardner TB, Chahal P, Papachristou GI, Vege SS, Petersen BT, Gostout CJ, et al. A comparison of direct endoscopic necrosectomy with transmural endoscopic drainage for the treatment of walled-off pancreatic necrosis. Gastrointest Endosc. 2009;69:1085–94.
- Rana SS, Bhasin DK, Sharma RK,Kathiresan J, Gupta R. Do the morphological features of walled-off pancreatic necrosis on endoscopic ultrasound determine the outcome of endoscopic transmural drainage? Endosc Ultrasound. 2014;3:118–22.
- Rana SS, Bhasin DK. Should all fluid collections in delayed phase of acute necrotizing pancreatitis labeled as walled-off pancreatic necrosis? Dig Dis Sci. 2014;59:1338–9.
- Talreja JP, Shami VM, Ku J, Morris TD, Ellen K, Kahaleh M. Transenteric drainage of pancreatic-fluid collections with fully covered self-expanding metallic stents (with video). Gastrointest Endosc. 2008 ;68:1199-203.