48uep6bbphidcol2|ID
48uep6bbphidvals|1808
48uep6bbph|2000F98CTab_Articles|Fulltext
Patients with recurrent or persistent abdominal pain as a result of pancreatic duct (PD) head strictures require treatment to achieve ductal decompression. Conventional retrograde PD decompression procedures such as pancreatic sphincterotomy, pancreatic stenting, and dilation of PD strictures are highly effective treatment options for these patients. In patients with either failed cannulation with conventional endoscopic retrograde cholangio-pancreatography (ERCP) or tight PD strictures, endoscopic ultrasonography (EUS)-guided PD drainage (EUS-PDD) has been described as a rescue option.
Case Report
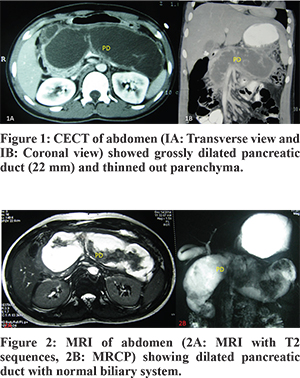
An 18-year-old boy presented with history of recurrent episodes of severe epigastric pain for one year being conservatively managed with analgesics. There was no history of biliary colic, passage of worms in stools, gastroenteritis, pancreatico-biliary intervention, jaundice, fever, steatorrhea, weight loss or diabetes mellitus. Transabdominal ultrasonography revealed dilation of pancreatic duct (PD) with parenchymal atrophy and calcification. Further, contrast enhanced computed tomography (CECT) of abdomen and magnetic resonance cholangio-pancreatography (MRCP) demonstrated grossly dilated PD of 22 mm and thinned out parenchyma of the entire pancreas (Figure 1,2). Side viewing endoscopy (SVE) showed a normal papilla and cholangiogram. However, cannulation of PD could not be done due to tight stricture in head of Pancreas.
Using an echoendoscope (GF-UC140P-AL5, Olympus, Japan) the dilated PD with echogenic content was visualized (Figure 3). Endoscopic pancreatico-gastrostomy was then performed under combined fluoroscopic and EUS guidance. A needle (19 G, Echo tip Ultrasound Needle, EUSN-19-T, Cook Ireland Ltd, Limerick, Ireland) was inserted across the stomach wall into the dilated proximal (upstream) pancreatic duct, dark brown fluid was aspirated. Aspirated fluid had high amylase levels (16000 IU/L), normal CEA level and cell count. A stiff guidewire (Metro, 0.035 inches) was placed into dilated PD. The track was dilated with 7F Sohendra Biliary Dilatation Catheter (SBDC) and 10 mm controlled radial expansion (CRE) balloon (Figure 4). Finally, a 10Fx7 cm double pigtail (DPT) plastic stent and 10F endoscopic naso-pancreatic drainage catheter (ENPD) was placed into the dilated PD. (Figure 4,5)
Patient remained asymptomatic after the procedure and repeat CECT of abdomen at 4 weeks revealed near normal pancreatic duct diameter with ENPD and DPT stents in situ (Figure 6). The patient is asymptomatic currently at 12 weeks of follow up.
Discussion
In patients of chronic pancreatitis with PD strictures, surgical drainage of the pancreatic duct has been shown to be superior to endoscopic treatment in various studies.1 However, surgical drainage is more invasive and has significant morbidity. Therefore, endoscopic treatment options need to be considered in patients. The standard endoscopic treatment for decompression of PD is via trans-papillary approach where successful cannulation via major papilla has been reported in 90-98% of cases.2 A few studies have demonstrated that EUS-guided transmural drainage of the PD is feasible in patients when conventional ERCP fails.3,4
The technical success rates of the EUS-guided rendezvous technique and PD stenting have been reported in two studies to be 77-92% and 25-100%, respectively.5,6 Several technical improvisations have been described to improve the success rate of EUS-guided PD drainage. Adjusting the direction of the needle before puncture allows greater success for appropriate PD decompression in pancreatic ductal hypertension-related benign PD strictures.
In conclusion, EUS-guided PD drainage is a feasible and useful treatment option for tight PD strictures to achieve ductal decompression, especially if transpapillary approach has failed. However, this procedure is technically challenging, requires expertise and has a high rate of complications, therefore should be performed preferably at tertiary care centers.
References
- Cahen DL, Gouma DJ, Nio Y, Rauws EA, Boermeester MA, Busch OR, et al. Endoscopic versus surgical drainage of the pancreatic duct in chronic pancreatitis. N. Engl J. Med. 2007;356:676–84
- Rosch T, Daniel S, Scholz M, Peterson BT, Levy MJ, Gostout CJ. Endoscopic treatment of chronic pancreatitis: A multicenter study of 1000 patients with long-term follow-up. Endoscopy. 2002;34:765–71.
- Will U, Meyer F, Manger T, Wanzar I. Endoscopic ultrasound assisted Rendezvous maneuver to achieve pancreatic duct drainage in obstructive chronic pancreatitis. Endoscopy. 2005;37:171–3.
- Mallery S, Matlock J, Freeman ML. EUS-guided rendezvous drainage of obstructed biliaryand pancreatic ducts: Report of 6 cases. Gastrointestinal. Endosc. 2004;59:100–7.
- François E, Kahaleh M, Giovannini M et al. EUS-guided Pancreaticogastrostomy. Gastrointest. Endosc. 2002;56:128–33.
- Bataille L, Deprez P. A new application for therapeutic EUS:Mainpancreatic duct drainage with a ‘pancreatic rendezvous technique’. Gastrointest. Endosc. 2002;55:740–3.