48uep6bbphidcol2|ID
48uep6bbphidvals|1801
48uep6bbph|2000F98CTab_Articles|Fulltext
Choledochal cysts have a female preponderance and may present late with cholangitis, pancreatitis or both in the adult age. Pancreas divisum may remain asymptomatic or present with pancreatitis. Riedel’s lobe may confuse clinically as a mass in the right hypochondrium mimicking a distended gallbladder or a choledochal cyst.We report a case of a 32-year-old lady who presented with recurrent episodes of pain abdomen and jaundice in whom a triple co-existence of a choledochal cyst, pancreas divisum and Reidel’s lobe was diagnosed.
Case Report
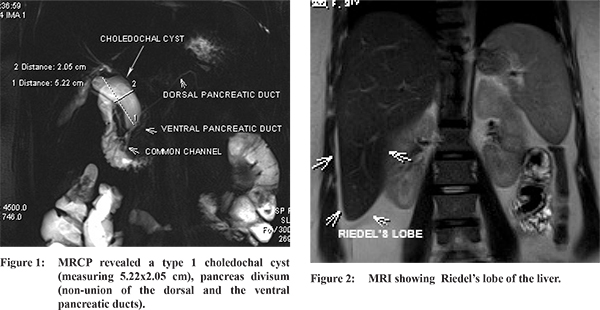
A 32-year-old lady presented with the history of recurrent upper abdominal pain and intermittent fever for two months. The patient was icteric and the abdominal examination revealed a palpable mass like impression in the right hypochondriumin continuity with the liver. Magnetic resonance cholangiopancreatography (MRCP) revealed a type 1 choledochal cyst (measuring 5.22x2.05 cm), pancreas divisum (non-union of the dorsal and the ventral pancreatic ducts) (Figure 1) and the Riedel’s lobe of the liver (Figure 2). The right lobe of liver measured 21 cm cephalocaudally at its maximum and the Riedel’s lobe measured 5 cm from the most inferior costal cartilage. The symptoms were due to cholangitis of choledochal cyst origin and excluded pancreatitis. Further on imaging, the elongated downward projection of right lobe of liver was confirmed to be a Riedel’s lobe and not a palpable choledochal cyst. Thus in this patient the pancreas divisum and the Riedel’s lobe were asymptomatic and only the choledochal cyst presented symptomatically in the adult age. The patient underwent excision of the choledochal cyst and hepaticojejunostomy, following which she had complete relief of symptoms.
Discussion
Choledochal cyst and pancreas divisum are congenital anomalies which may remain asymptomatic up to adult age. The co-existence of a choledochal cyst and pancreas divisum has been reported previously.
1 The co-occurrence of these two is related to the anomalous pancreaticobiliary ductal union (APBDU) during the rotation and fusion of the ventral pancreatic bud with the dorsal pancreatic bud which happens in the seventh week of embryogenesis, before they join the biliary tree. Any aberration of this process results in an APBDU. This can lead to anomalies such as choledochal cyst, pancreas divisum and pancreatic aplasia.
2 The incidence of choledochal cyst in the western population is 1 in 100 000-150 000 live births,
3 with higher incidence of 1 in 1000 in Asian populations.
4 The incidence of pancreas divisum is 3-7 % in endoscopic retrograde cholangiopancreatography series and 9% in autopsy series.
5 Riedel’s lobe is an asymptomatic condition with incidence variable from 3.3% to 31%.
6 The Riedel’s lobe and a choledochal cyst (palpable in 10-20 % of cases) can mimic each other as a mass in the right hypochondrium and may pose a diagnostic confusion, clinically.
References
- Dalvi AN, Pramesh CS, Prasanna GS, Rege SA, Khare R, Ravikiran CS. Incomplete pancreas divisum with anomalous choledochopancreatic duct junction with choledochal cyst. Arch Surg. 1999;134(10):1150-2.
- Tanaka T. Pathogenesis of choledochal cyst. Am J Gastroenterol. 1995:90:685.
- Gigot J, Nagorney D, Farnell M, Moir C, Ilstrup D. Bile duct cysts: A changing spectrum of disease. J Hepatobiliary Pancreat Surg. 1996;3:405-11.
- O’Neill JA Jr. Choledochal cyst. Curr Probl Surg. 1992;29:361-410
- Tadokoro H, Takase M, Nobukawa B. Development and Congenital Anomalies of the Pancreas. Anatomy Research International. 2011;2011:1-7.
- Gillard J, Patel M, Abrahams P, Dixon A. Riedel’s lobe of the liver: Fact or fiction? Clin Anat. 1998;11(1):47-49.