48uep6bbphidcol2|ID
48uep6bbphidvals|1747
48uep6bbph|2000F98CTab_Articles|Fulltext
Bochdalek hernia is the most common type of congenital diaphragmatic hernia (CDH) accounting for 81% of the total.
1 Usually, CDH is diagnosed by antenatal scanning or presents in the neonate with cardiorespiratory distress. However, few cases may remain dormant and may present in the adult with chronic vague abdominal or chest pain. Sometimes it may present with acute complications such as hollow viscus perforation, necrosis of its content, peritonitis, pancreatitis, gastric volvulus or incarceration of the colon which are very rare presentations. The exact incidence of adult Bochdalek hernia is difficult to calculate as most of these cases are asymptomatic and remain occult. About 100 cases of asymptomatic adult Bochdalek hernias have been reported inliterature.
2,3 We here in report the present case since literature describes only two previous cases of Bochdalek hernia in which gastric perforation and gastro-pleural fistula formation were found.
4,5
Case Report
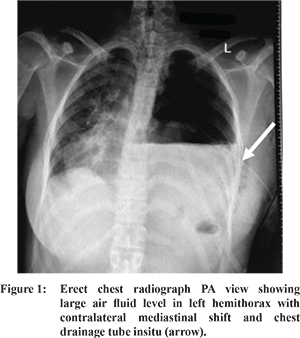
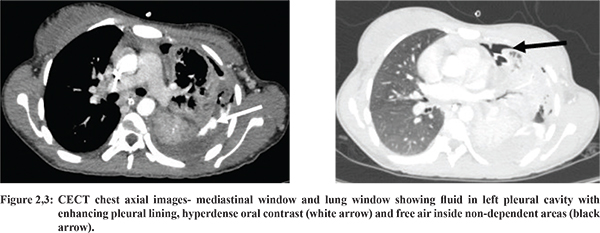
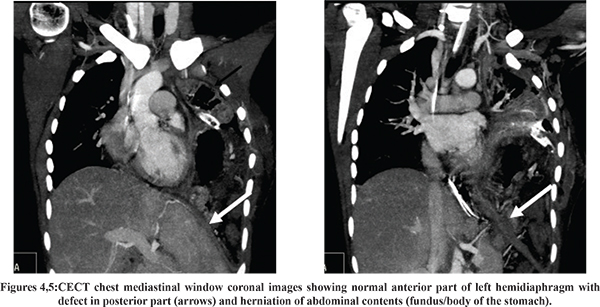
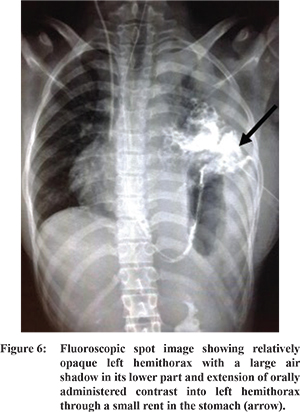
An 18-year-old female patient was referred to our emergency department with a history of left sided chest pain, fever and shortness of breath for 6 days. The pain was severe in intensity, pleuritic in nature, insidious and progressive and associated with nausea and vomiting. There was no previous history of chest or abdominal complaints. There were no known co-morbidities. There was no history of recent trauma or surgery. On physical examination, she was normotensive, febrile (1010F) and had tachycardia. There was fullness on the right side of the chest and the trachea was shifted to the right side. Breath sounds were diminished in the left axillary and mammary regions and absent in the left infra-axillary and infra-scapular areas. Per abdominal examination was within normal limits. The haemogram showed leucocytosis (11100/Cu mm).The initial chest X-ray showed hydropneumothorax on the left side with mediastinal shift (Figure 1). An intercostal tube drain was placed through the intercostal space. About 2000 ml of pus was drained out. The patient was relieved of dyspnoea, but pyopneumothorax with underlying collapsed lung was persistent on the repeat chest X-ray. So, the patient was referred to our institute for further management with a provisional diagnosis of broncho-pleural fistula or Boerhaave’s syndrome. Oxygen supplementation, injectable antibiotics and fluid resuscitation were continued. Fluid from the chest drainage tube showed elevated amylase and triglycerides levels. The patient revealed a history of vomiting and retching before the onset of the symptoms, so the possibility of Boerhaave’s syndrome with oesophago-pleural fistula was kept. In view of persistent fever, contrast enhanced CT scan of chest and abdomen was done with positive oral contrast. While administering contrast orally, the resident observed contrast coming through the intercostal tube drain. Contrast-enhanced computed tomography (CECT) chest revealed collapse of almost the entire left lung predominantly the lower lobe with mild hydro/pyopneumothorax with ICDT seen in-situ (Figure 2,3). Mild right-sided pleural effusion was also seen. The left hemidiaphragm was elevated with presence of a defect in the diaphragm measuring approximately 3.5 cm with herniation of the fundus/body of the stomach, spleen and tail of the pancreas into the left hemithorax. This was suggestive of perforation of the fundus of the stomach and gastro-pleural fistula formation (Figure 4,5). Non-ionic contrast administered orally was seen entering the left pleural cavity from the stomach, which was further confirmed by contrast fluoroscopy (Figure 6). Subsequently, the patient was taken up for surgery. A midline upper abdominal incision was given. Intra-operatively, the surgeon noted an 8x6 cm defect in the left posterior hemi-diaphragm with intra-thoracic herniation of the fundus and body of the stomach, entire spleen and the tail of the pancreas. The prolapsed stomach showed a 4x4 cm defect in the greater curvature adjacent to the fundus region and approximately 500 ml purulent fluid in the thoraco-abdominal cavity. The herniated contents were reduced and a splenectomy was performed. Primary repair of the gastric perforation was done. The diaphragmatic rent was repaired with Mersilk suture 2-0 without tension and mesh repair was avoided in view of pyothorax. The old chest drainage tube was replaced with a new one and peritoneal lavage was given. A feeding jejunostomy was done and drains were placed in the left sub-diaphragmatic region and the splenic fossa. Post-operative recovery was satisfactory.
Discussion
During the development of the diaphragm, pleural and peritoneal cavities communicate with each other through the patent pleuro-peritoneal canal which closes by the 9th to 10th week. When it remains patent in its posterolateral aspect and there is herniation of the abdominal content into the pleural cavity, the condition is called Bochdalek hernia. This entity was first described by Bochdalek in 1848. This can occur on both sides of the thorax. However, it is more common on the left side. It is the most common type of congenital diaphragmatic hernia. Usually, it presents in the neonatal period with cardiorespiratory distress. However, it may remain occult throughout life or may present in adulthood with chronic abdomino-thoracic discomfort. Sometimes in adults it may present acutely with hollow viscus perforation or intestinal obstruction. Major causes of a late acute presentation include trauma, physical exertion, pregnancy, labour, sneezing or coughing and sometimes, ingestion of large meals.6 Radiological imaging plays a vital role in early diagnosis in such patients as it is non-invasive. As surgery is the mainstay in the management of these patients, preoperative delineation of anatomy is very essential.
References
- Detti L, Mari G, Ferguson JE. Color Doppler ultrasonography of the superior mesenteric artery for prenatal ultrasonographic diagnosis of a left-sided congenital diaphragmatic hernia. J Ultrasound Med. 2001; 20:689-692.
- Adelman S, Benson CD. Bochdalek hernias in infants: Factors determining mortality. J Pediatr Surg. 1976;1:569-573.
- Mullins ME, Stein J, Saini SS, Mueller PR. Prevalence of incidental Bochdalek’s hernia in a large adult population. AJR Am J Roentgenol. 2001;177:363-6.
- Yoshizu A, Kamiya K. Diaphragmatic hernia complicated with perforated stomach during preganancy. Kyobu Geka. 2011;64(6):487-90.
- Dash S, Kodavala AK, Nayak SR, Rao KVR, Prasad ND, Sridurga S. Pyopneumothorax with an unusual etiology. IJCRR. 2013;5(10):76-83.
- Wilbur AC, Gorodetsky A, Hibbeln JF. Imaging findings of adult Bochdalek hernias. Clin Imaging. 1994;18:224-229.