Vikas Singla, Anil Arora, Pankaj Tyagi, Rinkesh K Bansal, Praveen Sharma, Naresh Bansal, Ashish Kumar
Department of Gastroenterology & Hepatology
Sir Ganga Ram Hospital, New Delhi, India
Corresponding Author:
Dr Anil Arora
Email: dranilarora50@hotmail.com
DOI:
http://dx.doi.org/10.7869/tg.328
48uep6bbphidcol2|ID 48uep6bbphidvals|1709 48uep6bbph|2000F98CTab_Articles|Fulltext Recurrent pancreatitis is a common clinical problem encountered by the gastroenterologist. Its common causes are gall bladder stones, biliary microliths, alcohol, early presentation of chronic pancreatitis and metabolic causes like hypercalcemia and hypertriglyceridemia. Rarely, it can be caused by pancreatic ductal obstruction due to an ampullary or pancreatic neoplasm. Recently, in one of our patients who presented with recurent acute pancreatitis, we found the cause to be a leiomyosarcoma, which is very rare in the pancreas and has not been described previously in literature as a cause of recurrent pancreatitis.
Case Report
A 45-year old lady presented in February 2012, with the complaint of recurrent abdmoinal pain of 5 years duration. She had no past history of any alcohol intake or of gall stone disease. The pain was epigastric in location with radiation to the back, and was associated with abdominal distension, obstipation and bilious vomiting without any history of jaundice, fever, gastrointestinal bleed, decreased urine output or dyspnoea. During the attacks of pain, levels of serum amylase and lipase would rise to more than 3 to 5 times the upper limit of normal. Contrast enhanced computed tomography done during the initial episode of pain revealed a dilated main pancreatic duct and a bulky pancreas without any evidence of pancreatic parenchymal calcification or mass in pancreas. Based on the biochemical and imaging findings, the patient was initially diagnosed as a case of chronic pancreatitis with recurrent episodes of acute exacerbations. Each episode of pain was treated with parenteral analgesics. The pain would last for two to five days and the patient was apparently healthy in between the atacks. The patient had had multiple episodes of pain over the previous 5 years, with a frequency of one or two episodes per year.
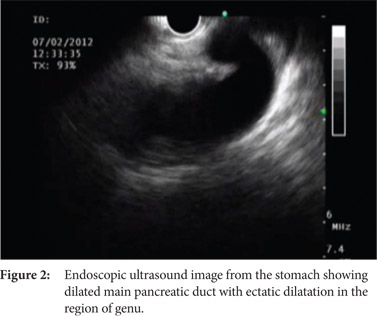
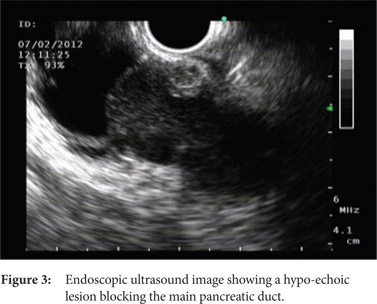
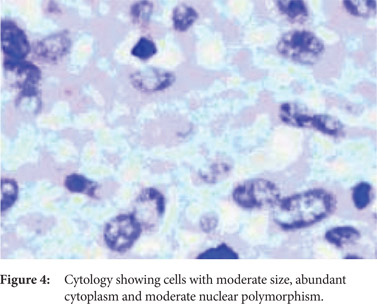
During the last such episode in February 2012, she presented to our hospital with the complaint of significant weight loss and persistent pain for more than 4 weeks. Her physical examination was unremarkable except for her low body mass index. Contrast enhanced CT scan revealed dilated main pancreatic duct with a 3 cm cyst in the head of the pancreas without any pancreatic calcification (Figure 1). On account of change in the nature of the pain and significant weight loss, the patient was planned for an endoscopic ultrasound examination for evaluation of the cystic lesion and to rule out pancreatic malignancy. Linear array echoendoscope (GFUCT180; Olympus Medical, Tokyo, Japan) was used for endosonography, which revealed dilated main pancreatic duct in the region of the pancreatic body and tail (Figure 2). The main pancreatic duct was ectatically dilated giving the appearance of a cyst in the pancreatic head. A hypoechoic lesion measuring 13x9 mm and blocking the main pancreatic duct was identified in the pancreatic head region, without any vascular invasion or enlargement of peri-pancreatic or peri-vascular lymph nodes (Figure 3). EUS examination of the common bile duct and liver was unremarkable. Transduodenal fine needle aspiration was performed with a 25 G needle (EchoTip Ultra, Cook Endoscopy, Winston Salem, NC, USA), and the sample was submitted for cytological examination. The report was suggestive of a tumour with papillary fragments, and the fragments were lined by 3 to 4 layers of cells with abundant cytoplasm and moderate nuclear polymorphism, consistent with the diagnosis of stromal cell tumor (Figure 4). Based on the imaging and cytological findings, a final diagnosis of recurrent acute pancreatitis secondary to pancreatic head stromal tumor was made, and the patient was subjected to curative surgery.

 Intra-operatively, the pancreatic duct was grossly dilated as it was blocked by the tumour in the pancreatic head, and the tumor was not invading surrounding vessels or tissues. Pylorus- preserving pancreaticoduodenectomy was done, and the post-operative course was uneventful. The patient was discharged on the 8th post-operative day. Histopathological examination revealed a 1.5x 1.0 cm greyish white tumor in the pancreatic head, which was blocking the main pancreatic duct. Sectioning showed a highly cellular tumour, with spindle, polygonal and oval cells, arranged in an interlacing pattern, and revealed that the tumour was arising from the main pancreatic duct wall. Immunostaining was positive for SMA and vimentin, and negative for CD 117, CK, CD 34, and myogenin (Figure 5). The duodenum, the rest of the intestine, and the resected margins were normal and free of tumour. Based on these findings, a final diagnosis of leiomyosarcoma of the pancreas arisng from the main pancreatic duct was established.
The patient has been under regular follow up for the last 2 years, and is free of all the previous symptoms.
Discussion
About 5%–7% patients with pancreaticobiliary tumors may present with acute pancreatitis. Common tumors presenting as acute pancreatitis include ampullary tumors and cystic neoplasms of the pancreas, especially the intra-ductal papillary mucinous tumour (IPMT).[1]
This is the first case report of leiomyosarcoma of the pancreas presenting as recurrent attacks of pancreatitis. Leiomyosarcoma in itself is a rare pancreatic tumor, but is the most common stromal tumor of the pancreas.[2] The clinical presentation of leiomyosarcoma is variable. The tumour usually presents in the fifth decade of life and males are affected more often than females . Abdominal pain and weight loss are the most commonly reported symptoms. The median size is more than 10 cm, and it can reach upto 25 cm. Large tumours can develop cystic degeneration and can mimic pseudocysts of the pancreas.[3] Leiomyosarcomas of the pancreas may invade adjacent structures and cause widespread metastasis to the liver and lung; however, lymphatic involvement is rare. Abdominal CT scan may reveal solid, cystic and heterogeneous lesions distributed along the pancreatic head, body and tail.
A definitive diagnosis may be established by histology, which is required to confirm its myogenic origin, and differentiate it from neurogenic and stromal tumors. The tumour cells are positive for desmin and smooth muscle actin, and negative for S-100 protein and CD117. Surgery is the curative treatment and the type of surgery depends on the site of the tumour. Pancreatic head tumors are treated by Whipple’s procedure, while tail tumors require distal pancreatectomy.
References
Intra-operatively, the pancreatic duct was grossly dilated as it was blocked by the tumour in the pancreatic head, and the tumor was not invading surrounding vessels or tissues. Pylorus- preserving pancreaticoduodenectomy was done, and the post-operative course was uneventful. The patient was discharged on the 8th post-operative day. Histopathological examination revealed a 1.5x 1.0 cm greyish white tumor in the pancreatic head, which was blocking the main pancreatic duct. Sectioning showed a highly cellular tumour, with spindle, polygonal and oval cells, arranged in an interlacing pattern, and revealed that the tumour was arising from the main pancreatic duct wall. Immunostaining was positive for SMA and vimentin, and negative for CD 117, CK, CD 34, and myogenin (Figure 5). The duodenum, the rest of the intestine, and the resected margins were normal and free of tumour. Based on these findings, a final diagnosis of leiomyosarcoma of the pancreas arisng from the main pancreatic duct was established.
The patient has been under regular follow up for the last 2 years, and is free of all the previous symptoms.
Discussion
About 5%–7% patients with pancreaticobiliary tumors may present with acute pancreatitis. Common tumors presenting as acute pancreatitis include ampullary tumors and cystic neoplasms of the pancreas, especially the intra-ductal papillary mucinous tumour (IPMT).[1]
This is the first case report of leiomyosarcoma of the pancreas presenting as recurrent attacks of pancreatitis. Leiomyosarcoma in itself is a rare pancreatic tumor, but is the most common stromal tumor of the pancreas.[2] The clinical presentation of leiomyosarcoma is variable. The tumour usually presents in the fifth decade of life and males are affected more often than females . Abdominal pain and weight loss are the most commonly reported symptoms. The median size is more than 10 cm, and it can reach upto 25 cm. Large tumours can develop cystic degeneration and can mimic pseudocysts of the pancreas.[3] Leiomyosarcomas of the pancreas may invade adjacent structures and cause widespread metastasis to the liver and lung; however, lymphatic involvement is rare. Abdominal CT scan may reveal solid, cystic and heterogeneous lesions distributed along the pancreatic head, body and tail.
A definitive diagnosis may be established by histology, which is required to confirm its myogenic origin, and differentiate it from neurogenic and stromal tumors. The tumour cells are positive for desmin and smooth muscle actin, and negative for S-100 protein and CD117. Surgery is the curative treatment and the type of surgery depends on the site of the tumour. Pancreatic head tumors are treated by Whipple’s procedure, while tail tumors require distal pancreatectomy.
References
- Kahrilas PJ, Hogan WJ, Geenen JE, Stewart ET, Dodds WJ, ?Arndorfer RC. Chronic recurrent pancreatitis secondary to a submucosal ampullary tumor in a patient with neurofibromatosis. Dig Dis Sci. 1987; 32:102–7.
- Baylor SM, Berg JW. Cross-classification and survival characteristics of 5000 cases of cancer of the pancreas. J Surg Oncol. 1973; 5:335-58.
- Sato T, Asanuma Y, Nanjo H, Arakawa A, Kusano T, Koyama K et al. A resected case of giant leiomyosarcoma of the pancreas. J Gastroenterol 1994; 29:223-7.
|