|
|
|
|
 |
|
| |
 |
|
|
Case Report |
|
|
|
|
|
Keywords :
|
|
|
where can i buy the abortion pill over the counter buy abortion pill
Department of Pathology1 and Surgery2,
Topiwala National Medical College and
B.Y.L Nair Hospital,
Mumbai-400008, India
Corresponding Author:
Dr. Parikh Jeenal Shailesh,
Email: parikh_jeenal@yahoo.co.in
DOI:
http://dx.doi.org/10.7869/tg.291
48uep6bbphidvals|1355 48uep6bbphidcol2|ID 48uep6bbph|2000F98CTab_Articles|Fulltext Invasive aspergillosis has emerged as a cause of severe infection in immune-compromised patients. The lungs are primarily affected, likely due to its portal of entry through the respiratory tract. Very few cases in the literature show primary involvement of the gastrointestinal tract.[1] Also disseminated aspergillosis in the immune-competent state is rare.[2-3]
Case report
A 70-year old male patient, admitted to our tertiary care hospital, had chief complaints of pain in abdomen and inability to pass stools for 8 days. He had no complaints of fever, nausea, vomiting, yellowish discoloration of urine or stools or any significant past surgical or medical history of tuberculosis, diabetes mellitus, hypertension or bronchial asthma. He was afebrile and conscious with pulse of 98 beats/min and blood pressure of 110/70 mmHg. His abdomen was distended and tender, with guarding and absent bowel sounds. His hemoglobin was 10.7 g/dL, WBC count of 10,700/mm3 (Polymorphs-89%, Lymphocytes-8%, Eosinophils-3%) and platelet count of 1.43 x105/mm3. Random blood sugar level was 167g/dL. The serology status of the patient was negative for HIV, HCV and HBsAg.
Ultrasonography of the abdomen showed distended bowel loops with gas shadows, suggestive of partial intestinal obstruction. Immediate emergency laparotomy showed 0.5 cm x 0.5 cm perforation, 50 cm proximal from the ileocaecal junction with dense adhesions and perforative peritonitis. A primary closure of the perforation site was performedwith drain in situ. The postoperative general condition was moderate and the patient was afebrile. But, a leak from the drain was noted. Re-exploration showed new serosal tear of the small intestine, for which primary suturing was done. His general conditions were stable. From post-operative day five, he developed intermittent spikes of high bloodpressure. Electrocardiogram showed depression in leads II and III.
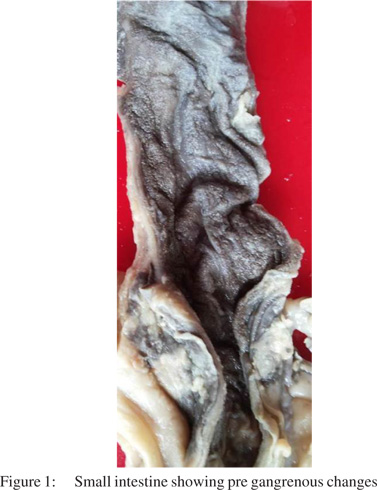
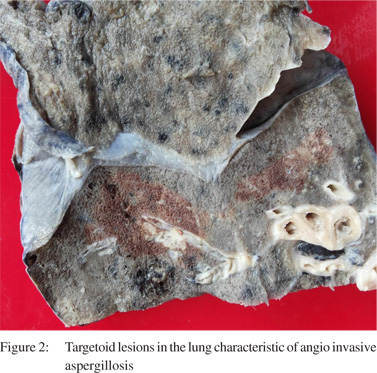
Troponin-T was positive. He developed pleural effusion with consolidation, bilaterally. WBC counts increased to 18,360/mm3. Tracheal SCAST was positive for Klebsiella pneumonia species. He died on twelfth post-operative day. At autopsy, the stomach fundus showed a large necrotic ulcer, with multiple small ulcers along its lesser curvature. Small and large intestine showed pre-gangrenous changes with serosa covered with greenish yellow exudates and thinned out, dusky mucosa containing altered blood (Figure 1). Also, the small intestine showed suture-site covered with similar exudates and few tiny small ulcers. Bilateral lungs showed target lesions, characteristic of angio-invasive aspergillosis
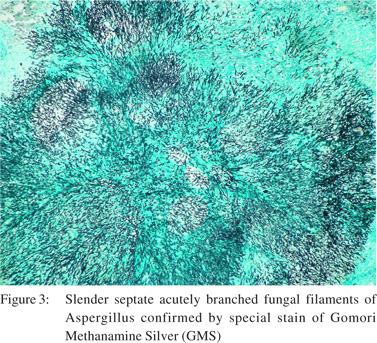
(Figure 2). The heart showed small endocardial vegetations with left anterior descending coronary artery showing 100% block. Liver and spleen capsules showed focal yellowish exudates. There was no focus of infection in the brain. Microscopy of the small intestine showed features of gangrene with perforation, superadded infection and the presence of slender septate, acutely branched fungal filaments of Aspergillus, which were further confirmed with special stain of Gomori Methanamine Silver (GMS) (Figure 3).
The lungs showed features of acute invasive aspergillosis with lung infarction and pulmonary vessels showing septic fungal fibrin thrombi. The cardiac vegetation, seen on gross examination, corresponded to septic infective endocarditis with the presence of few fungal filaments. The left anterior descending coronary artery showed an 80% fibro-calcific plaque. The liver and spleen capsules were thickened with moderate mixed inflammation.
The final cause of death was disseminated aspergillosis involving the gastrointestinal tract, lungs and heart with acute coronary insufficiency.
Discussion
Few reports in the literature show gastrointestinal aspergillosis, without pulmonary involvement as the initial presentation of disseminated disease.4 Involvement of extrapulmonary sites such as the skin, brain, gastrointestinal tract, heart and kidney are rare.
Gastrointestinal aspergillosis may be clinically asymptomatic or rarely present as a localized tumour like mass (aspergilloma) or as locally infiltrative lesions causing intestinal ischemia and obstruction. The gastro-intestinal tract can be involved via esophageal or bowel mucosal ulceration or via dissemination from a primary pulmonary aspergillosis. The aspergillus spores cannot survive in the normal gastric mucosa. However, ulceration and a necrotic tissue background provides a ready environment for the germinating spores. Many patients of gastrointestinal aspergillosis are asymptomatic. Invasive aspergillosis should be considered in the differential diagnosis of an otherwise undiagnosed febrile respiratory illness, even in immune-competent patients.[5]
Considering the acute course of the disease in our patient, it seems likely that gastro-intestinal aspergillosis preceded the pulmonary and cardiac aspergillosis. The gastro-intestinal ulcers may have been the primary site from which further infective dissemination may have occurred. Subsequently, these ulcers perforated and peritonitis developed. Also, there was no evidence of immunecompromised
status of our patient.
Thus, this is a very rare clinical presentation of fatal invasive aspergillosis in an immune-competent elderly male.
References
- Eggimann P1, Chevrolet JC, Starobinski M, Majno P, Totsch M, Chapuis B, Pittet D. Primary Invasive Aspergillosis of the Digestive Tract: Report of Two Cases and Review of the Literature. Infection. 2006;34:333–8.
- Ibrahim AH1, al Malki TA, Morad N. Primary locally infiltrative gastrointestinal aspergilloma in a non-neutropaenic child. JR Coll Surg Edinb. 2000;45:335–8.
- Imad M. Obeid, Sana Quddus, Geneva B. Tatem. Cerebral and pulmonary invasive disseminated aspergillosis in immunocompetent patient. Chest. October 2008, Vol 134, No. 4_Meeting Abstracts
- Shah SS, Birnbaum BA, Jacobs JE. Disseminated aspergillosis inciting intestinal ischaemia and obstruction. Br J Radiol. 2001;74:1145–7.
- Invasive aspergillosis in an immunocompetent patient with fever and a cardiac mass Matthew La Barbera, Lester B. Jacobson Infectious Disease Reports. 2011;3:62.
|
|
|
|
|
|