|
|
|
|
 |
|
| |
 |
|
|
Case Report |
|
|
|
|
|
Keywords :
|
|
|
Srikanth KP1, Thapa BR1, Sadhna B Lal1, Prema Menon2, Kushaljit Sodhi3, Kim Vaiphei4, Rao KLN2
Department of Pediatric Gastroenterology1,
Pediatric Surgery2, Radiology3, and
Histopathology4,
Post Graduate Institute of Medical Education and Research
Chandigarh-160012, India
Corresponding Author:
Prof Thapa BR
Email: brthapa1@yahoo.co.in
DOI:
http://dx.doi.org/10.7869/tg.271
48uep6bbphidvals|731 48uep6bbph|2000F98CTab_Articles|Fulltext Gastrointestinal duplications are congenital anomalies due to defective canalization of the GI tract. They may occur at any site from mouth to anus, but with variable frequency.[1] Gastric duplications are among the relatively rare duplications, and are usually difficult to diagnose and treat.We report here a case of gastric duplication, which presented as a large antral gastric ulcer with hematemesis.
Case: A 7-year old boy came to us with a history of periumbilical and epigastric pain abdomen, which started 2 years prior to presentation, and lasted for 6 months, and was being managed with proton pump inhibitors. There was no history of NSAID intake. Investigations including ultrasonography abdomen and contrast enhanced CT abdomen,which was unremarkable.A fresh episode of epigastric pain and recurrent non-bilious vomiting started one month prior to referral and was managed symptomatically. A day prior to admission he had 3 episodes of minor hematemesis, not requiring blood transfusion. On examination, he had normal anthropometry and was hemodynamically stable. Except for epigastric tenderness, systemic examination was normal. His hemoglobin was12.9g/dL, total leukocyte count: 8900/µL, platelet counts: 335000/µL and normal liver function tests. USG abdomen showed a cystic lesion in the gastro-hepatic ligament, in the antro-pyloric region along the lesser curvature (Figure 1). The CECT abdomen done 1.5 years agoreported normal at the time, when reviewed, showed the same lesion. Upper gastrointestinal endoscopy revealed a large antral ulcer with gastric wall edema (Figure 2).
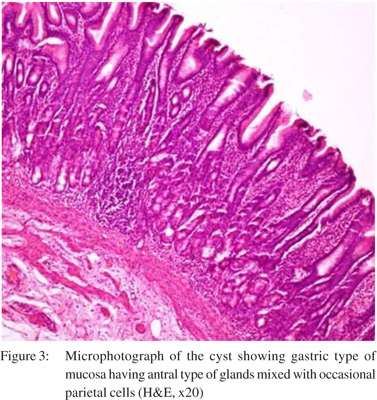
Evaluation for H.pylori was negative and serum gastrin assay was 74.6pg/mL (normal range 13-115pg/mL). He continued to be treated with PPIs and repeat endoscopy after 3 weeks just before surgery showed healing of the ulcer. Laparotomy revealed a gastric duplication cyst in the wall of the antrum of the stomach with no apparent internal communication. The patient underwent cyst excision along with adjacent stomach wall followed by end to transverse anastomosis of the pylorus and first part of the duodenum. Histopathological examination of the cyst was consistent with gastric duplication cyst (Figure 3). The post-operative period was uneventful and he was discharged on day 7 andnormal feeding advised. He has remained asymptomatic thereafter for 6 months at the time of reporting and repeat endoscopy revealed a normal gastric mucosa.


Discussion
Gastrointestinal duplications are rare GI anomalies with the frequency of 1 per 4500 live births, the ileum being the most common site followed by the foregut, least commonly seen in the tongue and pharynx1. Most children present before the age of one year, with symptoms depending on the site of involvement and associated complications.[1,2] Split notochord theory and incomplete recanalisation of the primitive gut have been postulated as the embryological basis for the development of the duplications.[3] They may be cystic or tubular; communicating or non-communicating. Cystic and noncommunicating ones are reported as more frequent than tubular and communicating duplications. The mucosa is usually the same as that of the adjacent normal bowel; however a different type of mucosal lining is not infrequent. Complications include gastrointestinal bleeding, secondary infection; compression of adjacent normal bowel; pain; and rarely malignant transformation has been noted in adults. Hemorrhage and infection tend to occur in communicating duplications.
Bleeding results due to ulceration of the surrounding normal mucosa by the gastric acid secreted by the mucosal lining.USG is considered an accurate investigative tool and frequently shows an aperistaltic bowel like structure with a lumen and an echogenic lining. However, contrast tomography/magnetic resonance imaging or even endoscopic ultrasonography (EUS) may help in the diagnosis if USG is non contributory. The 99m technetium pertechnates scan are also useful to pick up gastric mucosa lined duplication cysts. Excision is the treatment of choice as duplications will continue to be symptomatic unless removed. Isolated GI duplication has an excellent post surgery prognosis[4].Exact cause for large antral gastric ulcer is not known; however a rare physiological alteration similar to retained antral syndrome, a syndrome of uninhibited gastrin secretion and refractory gastric ulcers as seen after surgery for peptic ulcer disease has been contemplated[5].
References
- Gross RE, Holcomb GW, Farber S. Duplications of the alimentary tract. Pediatrics 1952;9:448–68.
- Bower RG, Sieber WK, Kiesewetter WB. Alimentary tract duplication in children. Ann Surg. 1978;188:669–74.
- Bentley JFR, Smith JR. Developmental posterior enteric remnants and spinal malformations. Arch Dis Child. 1960;35:76–86.
- Stringer MD, Spitz L, Abel R, Kiely E, Drake DP, Agrawal M, et al. Management of alimentary tract duplication in children. Br J Surg.1995;82,74–8.
- Gibril F, Lindeman RJ, Abou-Saif A, Shojamanesh H, Roy PK, Peghini PL, et al. Retained gastric antrum syndrome: a forgotten, treatable cause of refractory peptic ulcer disease. Dig Dis Sci 2001;46:610–7.
|
|
|
|
|
|