48uep6bbphidvals|705
48uep6bbph|2000F98CTab_Articles|Fulltext
Case
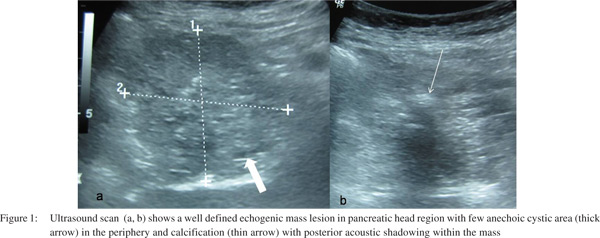
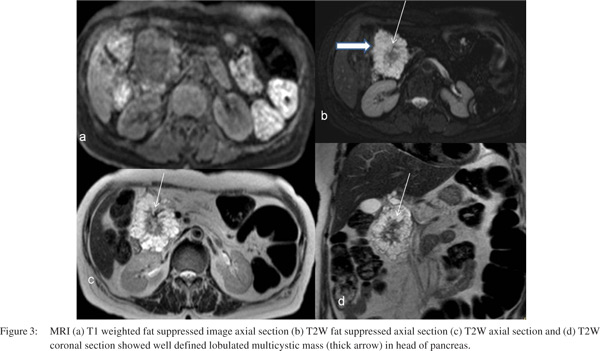
A 70-year-old female presented with occasional abdominal pain. There was no jaundice, loss of appetite, loss of weight or fever. She underwent transabdominal ultrasound (US) which showed well circumscribed lobulated echogenic mass in the pancreatic head region with peripheral anechoic cysts and foci of calcification (Figure 1). Multi-phase CT (MPCT) images showed well-defined lobulated hypodense mass composed of multiple cysts (more than 6 in number) of sizes less than 2cm with enhancing thin septation and calcified central stellate scar (Figure 2). The mass had a well-defined fat plane with the surrounding structures with no evidence of invasion or compression . There was fatty replacement of body and tail of pancreas with normal caliber main pancreatic duct (MPD). On MRI (Figure 3), the lesion was lobulated, and welldefined, present in the head of pancreas, composed of multiple, cysts and size less than 2cm appearing hypointense on T1W and hyperintense on T2W images with central area of T1 and T2 hypointensities suggestive of central stellate scar. The thin fibrous septations appeared hypointense on both T1W and T2W images. There was no evidence of diffusion restriction or signal drop on chemical shift imaging within the mass. No mural nodularity or solid component was seen within the mass. MPD was not seen to communicate with the mass.

Based on the typical radiological features on US, MPCT and MRI, diagnosis of microcystic serous cystadenoma of head of pancreas was made. Complete blood count, liver function test, amylase level, CA 19-9, CEA levels were within normal limits. The patient is on follow up.
Discussion
Serous cystadenoma of pancreas is a rare benign cystic neoplasm constituting 1-2% of all exocrine pancreatic tumors and isn’t it 10-15% of all cystic pancreatic neoplasms.[1] It is usually found incidentally on cross-sectional imaging done for other indications. It is more commonly seen in women (about 80%) older than 60 years and has also been referred to as grandmother lesion. They occur most commonly in the head of the pancreas with size range of few millimeters to 20cm. They have three typical morphological patterns: polycystic, honeycomb and oligocystic.[2] The polycystic variety accounts for 70% of total serous cystadenoma consisting of multiple cysts of more than six in number with size less than 2cm. Honeycomb pattern accounts for 20% and oligocystic which is also known as macrocystic variety has cysts of size more than 2cm and constitutes about 10%. Central stellate scar with calcification is seen in about 30% of the patients.[3] Giant tumors with ductal dilatation, intratumoral hemorrhages, solid variants, unilocular cystic form, interval growth and disseminated forms are atypical presentations of serous cystadenoma.[4] It is also associated with Von Hippel Lindau disease.
References
- Solicia E, Capella C, Kloppel G. Tumors of theexocrine pancreas. 3rd series, fasc. 20. In: Rosai J,Sorbin L, editors. Atlas of tumor pathology. Washington,DC: Armed Forces Institute of Pathology; 1997.p.31–144.
- Sarr MG, Murr M, Smyrk TC, Yeo CJ, Fernandez-del-Castillo C, Hawes RH,et al. Primary cysticneoplasms of the pancreas: neoplastic disordersof emerging importance—current state-oftheart and unanswered questions. J Gastrointest Surg.2003;7:417–28.
- Choi JY, Kim MJ, Lee JY, Lim JS, Chung JJ, Kim KW, et al.Typical and Atypical Manifestations of Serous Cystadenoma of thePancreas: Imaging Findings with Pathologic Correlation. AJR 2009;193:136–42.
- Dewhurst CE, Mortele KJ. Cystic Tumors of the Pancreas: Imaging and Management. Radiol Clin N Am. 2012;50:467–86.