48uep6bbphidvals|710
48uep6bbph|2000F98CTab_Articles|Fulltext
Isolated retroperitoneal retrovesical hydatid cyst is extremely rare with an incidence of 0.1/100,000 persons.[1]Hydatid cyst in the retrovesical area usually presents with pressure effects on adjacent organs such as urinary bladder and rectum.[2] We report a case of isolated retrovesical hydatid cyst (RVHC) presenting with obstructive uropathy and bilateral lower limb oedema. This type of presentation is extremely rare.
Case
A 36-year-old male patient presented with fullness and pain in the lower abdomen, and difficulty in passing urine of 3 weeks duration. There was straining and a sense of incomplete voiding. He also had bilateral lower limb edema, which had progressed over the same duration. There was no history of fever, trauma or any chronic illness. He was a farmer who kept livestock. The patient was in agonizing pain on arrival. His vital parameters were normal. Per abdominal examination showed fullness of lower abdomen with mild tenderness. Digital examination of rectum revealed a large, smooth, spherical mass anteriosuperior to the rectum. The prostate was normal. Bilateral lower limb edema was pitting in nature. Distal pulsations were intact. The patient was immediately catheterized. Approximately 1300 ml of clear urine was drained. On reassessment, there was a smooth, non-tender immobile mass reaching almost up to the umbilicus.
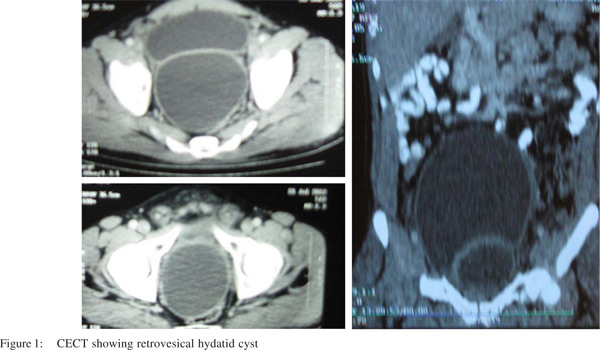
Lab parameters revealed normal hemoglobin with TLC-8300/mm3 (eosinophil-4%). Plain X ray chest and abdomen was normal. Retrograde urethrogram showed distended urinary bladder (UB). Ultrasound abdomen and pelvis showed a large cyst (14 cm ×10 cm ×14 cm) in the pelvis and hydronephrosis on the right side. CECT scan showed a large, non-enhancing, hypodense cystic lesion in the pelvis extending up to the coccyx and displacing the urinary bladder anterosuperiorly, compressing the rectum posterolaterally (Figure 1). Bilateral ureters were dilated with delayed contrast excretion.
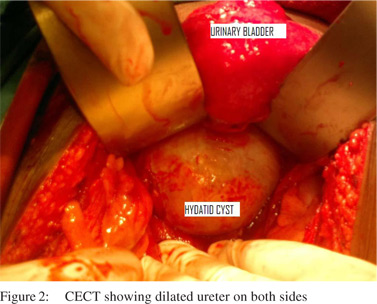
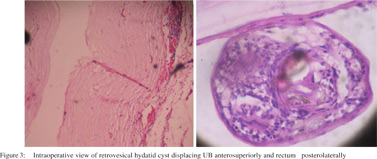
On laparotomy, there was a large cyst in the pelvis which lay beneath the pelvic peritoneum, displacing the rectum posteriorly and UB anterosuperiorly (Figure 3). The diagnosis of retroperitoneal retrovesical cyst was made. Cyst densely adhered to the adjacent retroperitoneal connective tissue and rectum. It was aspirated. Clear fluid was seen. Cytological examination demonstrated the presence of hooklets, confirming a hydatid cyst. 20% hypertonic saline was instilled into the cyst. After a few minutes, the fluid was reaspirated. An incision was made over the pericyst. The entire germinal layer of the hydatid cyst was removed. The pericyst was completely excised and sent for histopathological examination, which confirmed the diagnosis (Figure 3). The postoperative period was uneventful. Lower limb oedema subsided drastically immediately postop . He was discharged on the 5th postoperative day and advised a 4-week course of albendazole therapy (15mg/kg/day). Follow up ultrasonography after 15 days showed normal kidneys with no back-pressure changes. A total of 3 cycles of albendazole therapy was given with at 2- week intervals. The patient is symptom free after 15 months.
Discussion
Isolated retrovesical hydatid cyst (RVHC) is an exceptional occurrence. Aydinli et al from Turkey retrospectivelyanalyzed 653 surgically treated patients of intraabdominal hydatid cysts in 25 years(1979 to 2004)and found only one case in the retrovesical space.[3]
The challenge in managing these patients is the accurate preoperative diagnosis of hydatid disease. The sensitivity of ultrasonography and CT are 93-98% and 97% respectively. The sensitivity of serological test (Indirect hemagglutination test) is 87.5%only[4].
Treatment is primarily surgical i.e.complete removal of the entire cyst without contamination of the field. Robotic assisted laparoscopic surgery is the most recently introduced modality in the treatment of retrovesical hydatid cyst.
References
- Angulo JC, Escribano J, Diego A, Sanchez-Chapado M. Isolated retrovesical and extrarenal retroperitoneal hydatidosis: clinical study of 10 cases and literature review. J Urol. 1998;159:76–82.
- Horchani A, Nouira Y, Chtourou M, Kacem M, Safta ZB. Retrovesical Hydatid Disease: A Clinical Study of 27 Cases. Eur Urol. 2001;40:655–60.
- Aydinli B, Ozturk G, Polat KY. Extravisceral primary hydatid cyst of the retroperitoneum. ANZ J Surg. 2007;77:455–9.
- Balik A, Çelebi F, Baþoðlu M, Ören D,Yildirgan I, Atamanalp S. Intra-abdominal extrahepatic echinococcosis. Surg Today. 2001;31:881–4.
- Dogra P, Javali T, Saini A, Sharma S, Gupta N. Isolated retrovesical hydatid cyst. BJUI online DOI: 10.1002/BJUIw-2010–019.