Jayant K Ghosh, Sundeep K Goyal, Manas K Behera, Abhilash VB, Vinod K Dixit, Ashok K Jain
Department of Gastroenterology
Institute of Medical Sciences,
Banaras Hindu University,
Varanasi, India
Corresponding Author:
Dr. Jayant Kumar Ghosh
Email: drjayantkg@yahoo.co.uk
DOI:
http://dx.doi.org/10.7869/tg.253
48uep6bbphidvals|711 48uep6bbph|2000F98CTab_Articles|Fulltext Duplications of the gastrointestinal tract (GIT) are infrequent in the general population with an incidence of two or three cases per year in referred pediatric hospitals and more often discovered in the first two years of life.[1] This case study highlights tubular duplication of the transverse colon in an adult presenting with chronic diarrhea.
Case report
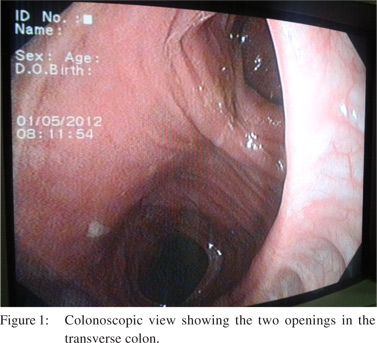
A 48 years old male came to our outpatient department with the chief complaint of chronic diarrhea for last 6 months. Clinical examination and routine investigations were unremarkable. Stool routine microscopy was normal and negative for any cyst, ova or parasite. Screening for HIV was negative. Serum anti-tissue transglutaminase was within normal limits. Upper GI endoscopy was normal. Colonoscopy revealed two luminal openings in the transverse colon just proximal to the splenic flexure. The colonoscope was passed through both openings (Figure 1). The mucosa in both the lumens appeared normal. Biopsy was taken to rule out heterotopia. The distal openings were seen in the transverse colon distal to hepatic flexure. The rest was normal. Barium enema showed the lumen communicated with the transverse colon at both ends. Patient was advised rifaximin 550 mg twice daily for 14 days and he showed improvement in diarrheal frequency. Rifaximin therapy was prolonged for a total of 4 weeks. Patient showed gradual improvement over the next 4 weeks. He became asymptomatic and remained so for the last 6 months. Patient was advised for regular colonoscopic surveillance for colorectal cancer.
Discussion
GIT duplication is rare and reported mostly in the pediatric age group. GIT duplication has been defined by Rowling’s criteria as: [1] the wall of the duplication is in continuity with one of the duplicated organ; [2] the cyst is surrounded by a smooth muscular layer; and [3] a layer of digestive mucosa is present, more often typical or heterotopic as gastric mucosa, colonic mucosa, bronchial or pancreatic structure.[2] The most frequent localization is ileum in 30% or ileocecal valve in 30% followed by jejunum in 8%, colonin 6%-7% and rectum in 5%.[3] If no associated malformation is present, they frequently remain hidden for several years until a complication occurs.[4] The symptoms are non-specific and depend on the type of duplication and the associated abnormality. More often they present as abdominal mass, chronic pain, constipation, obstruction, and less frequently volvulus, intussusception, bleeding, or perforation (especially in sigmoid colon mimicking diverticulitis). Carcinoma may arise: the most frequent is adenocarcinoma.[5]
References
- Blickman JG, Rieu PH, Buonomo C, Hoogeveen YL, BoetesC. Colonic duplications: clinical presentation and radiologicfeatures of five cases. Eur J Radiol. 2006;59:14–9.
- Rowling JT. Some observations on gastric cysts. Br J Surg.1959;46:441–5.
- Kekez T, Augustin G, Hrstic I, Smud D, Majerovic M, Jelincic Z, et al. Colonic duplication in an adult who presented with chronic constipation attributed to hypothyroidism. World J Gastroenterol. 2008;14:644–6.
- Mourra N, Chafai N, Bessoud B, Reveri V, Werbrouck A, Tiret E. Colorectal duplication in adults: report of seven cases and review of the literature. J Clin Pathol. 2010;63:1080–3.
- Hattori H. Adenocarcinoma occurring just at the attached site of colonic duplication in an adult man. Dig Dis Sci. 2005;50:1754.
|