Tejal Bhoy, Shailendra Lalwani, Jitendra Mistry, Vibha Varma, Vinay Kumaran, Samiran Nundy, Naimish Mehta
Department of Surgical Gastroenterology and Liver Transplantation
Sir Ganga Ram Hospital, New Delhi - 110060
Corresponding Author:
Dr Samiran Nundy
Email: snundy@hotmail.com
DOI:
http://dx.doi.org/10.7869/tg.225
48uep6bbphidvals|683 48uep6bbph|2000F98CTab_Articles|Fulltext Gastrointestinal stromal tumors (GIST) are uncommon, representing 0.1-3.0% of all gastrointestinal cancers. A primary GIST in the liver is even less frequent. We report a primary, malignant, hepatic gastrointestinal stromal tumor that was resected from the liver of a 41-year-old woman.
Case report
A 41-year-old female patient without any comorbidity, presented with a seven month history of pain in her right hypochondrium and right lower chest which was gradual in onset, severe, non-colicky and radiated to her back. It was not related to food intake and usually relieved with analgesics. She had lost approximately 6 kg bodyweight over the last 6 months and had anorexia since 3 months. Her medical history included an open cholecystectomy 16 years ago and abdominal tuberculosis 26 years back for which she completed a course of anti-tubercular therapy.
An ultrasound examination of her abdomen revealed a 6 × 5 cm mass in the right lobe of liver and fine needle aspiration cytology suggested a possible malignancy. Her serum alphafetoprotein was 23.3 ng/ml, and her viral markers were nonreactive.
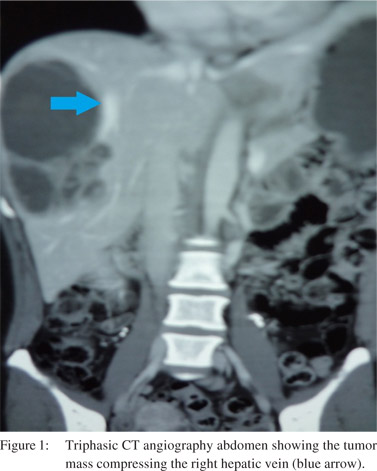
A triphasic CT angiography of the abdomen (Figure 1), revealed a 15 × 12 cm, heterogeneous mass lesion in the right lobe of liver, involving segments VI and VII, with cystic degeneration. The mass was compressing the right hepatic vein. There was a small satellite nodule in segment V.
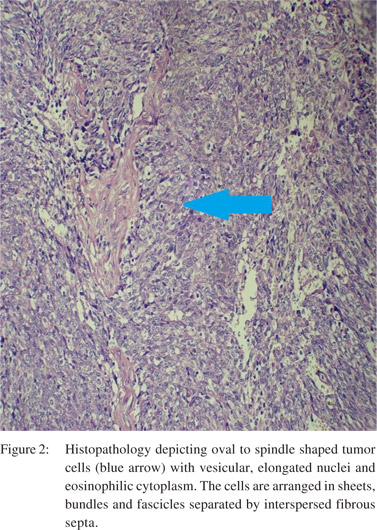
Intra-operative findings revealed a large lesion involving segmentsVI and VII of the liver with central necrosis and a cystic component. There was a4 × 3 cm lesion as well in segment Vwithout any free fluid, peritoneal nodules or pelvic deposits. The patient underwent a right hepatectomy. Her post-operative course was uneventful and she was discharged four days after surgery. Histopathology (Figures 2) showed oval to spindle shaped tumor cells with vesicular, elongated nuclei and eosinophilic cytoplasm. These were arranged in sheets, undles and fascicles separated by fibrous septa at places. Prominent cystic degeneration, areas of myxoid change and necrosis were also found. On immunohistochemistry (Figure 3) the tumor cells were strongly positive for CD117 and focally for SMA, but were negative for Hep-par 1 and vimentin. She was started on imatinib, buthad to be stopped due to its side effects. At 5-month follow-up, the patient is doing well without any recurrence.
 Discussion
Gastrointestinal stromal tumorsare the most common mesenchymal neoplasms of the GI tract. They are defined as spindle cell, epithelioid or occasionally pleomorphic, mesenchymaltumorsthat arise from the gastrointestinal tract and usually express the KIT protein. Stomach (40–60%) and small intestine (30–40%) are the most common sites of affliction. The colon, rectum, oesophagus, appendix,[1] and rarely the mesentery and retroperitoneum are other sites of origin. Very few cases of hepatic GIST have been reported.Regardless of where they occur, almost all GIST have the same biological behavior marked by expression of c-kit (CD117) protein.C-kit is a transmembrane growth factor receptor with tyrosine kinase activity, which helps differentiate these tumors from other mesenchymal tumors.Surgery is the best and only curative option. GIST rarely metastasize to the lymph nodes, so formal lymphadenectomy is not necessary. There are only three case Figure 3: Immunohistochemistry showingtumor cells strongly positive for CD117 and focally for SMA. reports of hepatic GIST in the literature, of which two underwent hepatectomy and one radiofrequency ablation therapy.[2-4]
References
Discussion
Gastrointestinal stromal tumorsare the most common mesenchymal neoplasms of the GI tract. They are defined as spindle cell, epithelioid or occasionally pleomorphic, mesenchymaltumorsthat arise from the gastrointestinal tract and usually express the KIT protein. Stomach (40–60%) and small intestine (30–40%) are the most common sites of affliction. The colon, rectum, oesophagus, appendix,[1] and rarely the mesentery and retroperitoneum are other sites of origin. Very few cases of hepatic GIST have been reported.Regardless of where they occur, almost all GIST have the same biological behavior marked by expression of c-kit (CD117) protein.C-kit is a transmembrane growth factor receptor with tyrosine kinase activity, which helps differentiate these tumors from other mesenchymal tumors.Surgery is the best and only curative option. GIST rarely metastasize to the lymph nodes, so formal lymphadenectomy is not necessary. There are only three case Figure 3: Immunohistochemistry showingtumor cells strongly positive for CD117 and focally for SMA. reports of hepatic GIST in the literature, of which two underwent hepatectomy and one radiofrequency ablation therapy.[2-4]
References
- Miettinen M, Majidi M, Lasota J. Pathology and diagnostic criteria of gastrointestinal stromal tumors (GISTs): a review. Eur J Cancer. 2002;38:S39–51.
- Hu X, Forster J, Damjanov I. Primary malignant gastrointestinal stromal tumor of the liver. Arch Pathol Lab Med. 2003;127:1606–8.
- Ochiai T, Sonoyama T, Kikuchi S, Ikoma H, Kubota T, Nakanishi M, et al. Primary large gastrointestinal stromal tumor of the liver: report of a case. Surg Today. 2009;39:633–6.
- Luo XL, Liu D, Yang JJ, Zheng MW, Zhang J, Zhou XD. Primary gastrointestinal stromal tumor of the liver: a case report. World J Gastroenterol. 2009;15:3704–7.
|