|
|
|
|
 |
|
| |
 |
|
|
Case Report |
|
|
|
|
|
Keywords :
|
|
|
Bhupendra Kumar Jain, Pankaj Kumar Garg, Dakid Palmo, Debajyoti Mohnaty, Vivek Agrawal
Department of Surgery,
University College of Medical Sciences
and Guru Teg Bahadur Hospital,
University of Delhi,
New Delhi - 110095, India
Corresponding Author:
Dr. Bhupendra Kumar Jain
Email: bhupendrakjain@gmail.com
DOI:
http://dx.doi.org/10.7869/tg.235
48uep6bbphidvals|693 48uep6bbph|2000F98CTab_Articles|Fulltext The scarcity of trained medical professionals continues to be a major concern in developing countries. Lack of stringent regulations permits quacks to impersonate as physicians and administer unscientific and potentially harmful treatment to gullible patients. Even in the 21st century, we continue to come across anorectal complications arising from unscientific management of haemorrhoids by quacks. Quacks are known to inject corrosive preparations in anal fistula as remedy.
However such quackery often leads to various local complications including necrotizing fasciitis of the perineum and scrotum, and systemic complications like septicemia and renal failure due to systemic absorption of chemical agents.[1] We report a case of complete anal obliteration following application of a corrosive preparation into the anus by a quack doctor for hemorrhoids, and describe its successful management at our hospital.
Case report
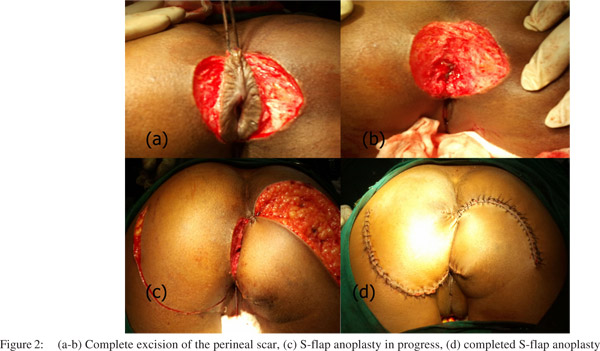
A 25-year-old lady presented with pain, distension of abdomen, and constipation of seven days duration. One month ago, the lady had applied a corrosive preparation into the anus on advice of a quack doctor, purportedly for the treatment of hemorrhoids. Soon after, she felt intense pain which subsided gradually; however, progressive constipation ensued. Abdominal examination revealed features of intestinal obstruction. A scar measuring 6.5 × 2.5 cm was found at the anus and the anus itself was obliterated (Figure 1a). Abdominal roentgenography showed dilated small and large bowel loops with multiple airfluid levels. MRI of the pelvis revealed a hugely dilated rectum with obliteration of the distal anal canal. An emergency loop transverse colostomy was performed to relieve intestinal obstruction. Two weeks later, central part of the perineal scar was incised to expose the lumen of anus, and the scar edge was sutured to the anal mucosa (Figure 1b). The obliteration was confined to distal one centimeter of the anal canal. Regular manual anal dilatation was performed using metallic dilators. After 4 months, the anal opening still remained inadequate in size, and it was non-distensible. Complete excision of the scar and reconstruction of anus by S-flap anoplasty was undertaken (Figure 2). Six weeks after surgery, digital rectal examination and anoscopy revealed complete healing. The new anus was found to be of adequate size, and it was distensible. Two months later, the loop colostomy was taken down and bowel continuity was restored. At follow up after ten months, the patient was well and she had no complaints of anal incontinence or constipation.

 Discussion
Extensive search of English literature failed to retrieve any previous reports of anal obliteration in adults. However, bkj there are cases of anal stenosis reported in the literature. Hemorrhoidectomy is reported as the most common cause (90%) of anal stenosis, followed by infections (tuberculosis, venereal diseases, etc.), inflammatory bowel disease and radiotherapy. We also searched for reports of anal injury caused by corrosive/caustic chemicals. Pubmed search strategy (“Anal” [All Fields] OR “anus” [All Fields]) AND (“stenosis” [All Fields] OR “obliteration” [All Fields]) AND (“caustics”[MeSH Terms] OR “caustics”[All Fields] OR “corrosive”[All Fields] OR caustics”[Pharmacological Action]) (accessed on 17.10.2012) retrieved only four previous reports of corrosive injury of the anorectum. da Fonseca et al[2] reported two cases of acute proctocolitis caused by rectal application of caustic products used for domestic purpose. Both these patients were prescribed symptomatic treatment.
Discussion
Extensive search of English literature failed to retrieve any previous reports of anal obliteration in adults. However, bkj there are cases of anal stenosis reported in the literature. Hemorrhoidectomy is reported as the most common cause (90%) of anal stenosis, followed by infections (tuberculosis, venereal diseases, etc.), inflammatory bowel disease and radiotherapy. We also searched for reports of anal injury caused by corrosive/caustic chemicals. Pubmed search strategy (“Anal” [All Fields] OR “anus” [All Fields]) AND (“stenosis” [All Fields] OR “obliteration” [All Fields]) AND (“caustics”[MeSH Terms] OR “caustics”[All Fields] OR “corrosive”[All Fields] OR caustics”[Pharmacological Action]) (accessed on 17.10.2012) retrieved only four previous reports of corrosive injury of the anorectum. da Fonseca et al[2] reported two cases of acute proctocolitis caused by rectal application of caustic products used for domestic purpose. Both these patients were prescribed symptomatic treatment.
Despite
persistent fibrosis in the lamina propria, no signs of stenosis were found in either of these patients. Pol et al[3] described a case of caustic rectal stenosis due to abuse of analgesic suppositories. They excluded the stenosis by distal colostomy. Subsequently, the stenosis appearing as a complete diaphragm was re-canalized using an EEA stapler. Ribault et al[4] reported case of extensive rectosigmoid stenosis which developed after potassium enema administered to a chronically constipated 26-year-old African woman. The patient was successfully managed by resecting the affected bowel and restoring continuity by performing trans-anal recto-colonic anastomosis. Non-operative management of anal stenosis includes sufficient fluids, fiber supplements, and stool softeners. Daily digital or mechanical anal dilatation may also prove helpful in mild stenosis. Operative management comprises of lateral internal sphincterotomy and formal anoplasty.[5] A number of anoplasty techniques have been developed based on the severity of stenosis, length of stenotic segment, and location of the stenosis. Our patient was managed using a step wise approach. Perineal scar was initially incised, and marsupialization was undertaken to restore the patency of anus. This allowed fair assessment of the length of the obliterated segment, and evacuation of collected feces from distal bowel. Regular dilatation failed to restore an anal opening of adequate size and distensibility. S-shaped rotation flap was required to create a new anus and cover the large raw area resulting from complete excision of the perineal scar. The S-flap anoplasty is used for the treatment of Bowen’s disease or Paget’s disease, where a large amount of skin has to be excised and new skin rotated into the area. In the prone position, a full-thickness Sshaped flap comprising of perianal skin, with the size of the base as great as its length, starting from the dentate line for approximately 8 cm to 10 cm is rotated and sutured to the normal mucosa after the scar tissue has been excised.[6,7]
Conclusion
Patients need to be protected from quacks by making them aware of safe remedies available in modern medicine for anorectal ailments. S-flap anoplasty is an appropriate rotation advancement procedure for the successful management of distal anal obliteration.
References
- Gupta PJ. The role of quacks in the practice of proctology. Eur Rev Med Pharmacol Sci. 2010;14:795–8.
- da Fonseca J, Brito MJ, Freitas J, Leal C. Acute colitis caused by caustic products. Am J Gastroenterol. 1998;93:2601–2.
- Pol B, Christophe M, Touchet J, Jacquin C, Maillot A. [Caustic rectal stenosis. Trans-anal resection using an EEA stapler]. Presse Med. 1993;22:1139–41.
- Ribault L, Carli P, Gabet J, Martet G, Gournier JP. [Extensive rectosigmoid stenosis caused by caustic enema. Apropos of a case in an African woman]. J Chir (Paris). 1988;125:650–3.
- Brisinda G, Vanella S, Cadeddu F, Marniga G, Mazzeo P, Brandara F, et al. Surgical treatment of anal stenosis. World J Gastroenterol. 2009;15:1921–8.
- Pearl RK, Hooks VH, 3rd, Abcarian H, Orsay CP, Nelson RL. Island flap anoplasty for the treatment of anal stricture and mucosal ectropion. Dis Colon Rectum. 1990;33:581–3.
- Ferguson JA. Repair of Whitehead deformity of the anus. Surg Gynecol Obstet. 1959;108:115–6.
|
|
|
|
|
|