|
|
|
|
 |
|
| |
 |
|
|
Case Report |
|
|
|
|
|
Keywords :
|
|
|
Mahendra Singh, Ashwani Gupta, ASN Rao, U Prashanth, Ashish Kumar
Department of Surgery, VMMC
Safdarjang Hospital,
New Delhi - 110017, India
Corresponding Author:
Dr. Mahendra Singh
Email: dr.mahi1118@gmail.com
DOI:
http://dx.doi.org/10.7869/tg.198
48uep6bbphidvals|657 48uep6bbph|2000F98CTab_Articles|Fulltext Intra-gastric knotting of nasogastric tube is a rare complication associated with deep insertion of a small bore tube.[1,2] Various provoking factors for knotting have been described.[3,4] We focus on prevention and management of this condition and report a case of spontaneous “lariat loop” knotting of a large bore nasogastric tube in the absence of any provoking factor.
Case report
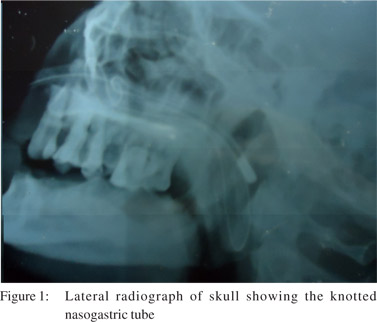
A 40-year-old male presented to the emergency department with small bowel obstruction. With the patient’s head flexed, a well lubricated 16 French nasogastric tube was inserted blindly through the left nostril in the first attempt without any difficulty. Proper placement was confirmed by auscultation over the stomach while injecting 20 ml air with a disposable syringe into the nasogastric tube and also by aspiration of gastric contents As the patient improved, it was decided to remove the nasogastric tube after three days. While attempting removal we experienced significant resistance near the end of the tube and were unable to retrieve it. The patient developed epistaxis and severe pain. A skull radiograph was performed which showed a knotted nasogastric tube (Figure 1). Using topical anaesthesia and laryngoscope, the distal knotted part, visible in the oropharynx, was grasped with a Magill forceps and pulled out of the mouth. On inspection, the tube was found to have developed a perfect “lariat loop” knot at its end (Figure 2).

Discussion
The nasogastric tube is commonly used for decompression of stomach and for enteral feeding in medical practice. Sometimes, this safe and innocent-looking tube can cause unexpected complications.[1] Complications include ulceration, bleeding, misplacement of the tube in the airway, and clogging and knotting of the tube.[1] Factors which predispose to knotting include narrow bore tubes, multiple manipulations during insertion, deep insertion into the stomach, a small stomach following gastroplasty, softening of the tube at body temperature and interference with an endotracheal tube in an intubated patient.[3,4] Knotting can lead to serious complications including respiratory distress, severe laryngeal injury and tracheoesophageal puncture.[3,5] Cases reported earlier have been associated with one or more risk factors. In our patient, none of the above mentioned risk factors were present. Knotting can prevented by using standard procedures and manoeuvres designed to facilitate easy insertion, such as using a wide bore tube, cooling the tube, good lubrication, inserting a Fogarty catheter through a suction port of the tube to increase its rigidity, forward displacement of the larynx, lateral neck pressure, direct guidance with two fingers in the mouth, and the use of Magill forceps under direct laryngoscopic visualization.[6-8] Proper tube length is estimated by measuring the distance from the nose to the pinna and from the pinna to the xiphoid process and adding 5cm.[3] Any difficulty during insertion or removal of a nasogastric tube should prompt immediate investigation to rule out possible knotting.[9]
Excessive traction should be avoided to prevent further tightening of the knot.[9] A skull radiograph can be performed to look for a knotted tube. Endoscopy is useful for both confirmation and retrieval. After confirmation, the knotted tube can be retrieved either by the nasal or oral route. For retrieval through nasal route, a 7.5 mm red nasopharangeal tube is passed over the nasogastric tube after adequate lubrication of the nostrils with lignocaine gel. The nasopharyngeal tube is pushed down the nostril while maintaining adequate tension over the nasogastric tube.[3] After adequate insertion, the knot can be pulled into the lumen of the nasopharyngeal tube and both tubes are removed nasally.[3] For oral retrieval, either general or adequate topical anaesthesia can be used depending on the patient’s condition. Under vision, the distal knotted part is grasped with a Magill forceps and is pulled out of the mouth after cutting the proximal part free.[9] We retrieved the knotted tube through the oral route.
References
- Baskin WN. Acute complications associated with bedside placement of feeding tubes. Nutr Clin Pract. 2006;21:40–55.
- Dasani B, Sahdev P. Knotting of a nasogastric tube: a case report. Am J Emerg Med. 1991;9:565.
- Dinsmore RC, Benson JF. Endoscopic removal of a knotted nasogastric tube lodged in the posterior nasopharynx. South Med J. 1999;92:1005–7.
- Santhanam V, Margarson M. Removal of self-knotted nasogastric tube: technical note. Int J Oral Maxillofac Surg. 2008;37:384–5.
- Malik NW, Timon CI, Russel J. A unique complication of primary tracheoesophageal puncture: knotting of the nasogastric tube. Otolaryngol Head Neck Surg. 1999;120:528–9.
- Ozer S, Benumof JL. Oro- and nasogastric tube passage in intubated patients: fiberoptic description of where they go at the laryngeal level and how to make them enter the esophagus. Anesthesiology. 1999;91:137–43.
- Perel A, Ya’ari Y, Pizov R. Forward displacement of the larynx for nasogastric tube insertion in intubated patients. Crit Care Med. 1985;13:204–5.
- Lind LJ, Wallace DH. Submucosal passage of a nasogastric tube complicating attempted intubation during anesthesia. Anesthesiology. 1978;49:145–7.
- Melki I, Matar N, Maalouf S, Rassi S. Knotting of nasogastric tube around a nasotracheal tube: An unusual cause of hypercapnia in a 3-month-old infant. Am J Crit Care. 2010;19:198–7.
|
|
|
|
|
|