Neeraj Nagaich, Prachis Ashdir, Rupesh Kumar Pokharna, Subhash Nepalia
Department of Gastroenterology,
SMS Medical College, Jaipur, India
Corresponding Author:
Dr. Rupesh Kumar Pokharna
Email: rkpokharna2@rediffmail.com
DOI:
http://dx.doi.org/10.7869/tg.193
48uep6bbphidvals|652 48uep6bbph|2000F98CTab_Articles|Fulltext Epiploic appendages are visceral peritoneal out-pouchings of colon containing fat and blood vessels. Appendagitis is a benign and self-limiting condition of epiploic appendages.[1] Primary epiploic appendagitis (PEA) results from spontaneous thrombosis of the veins draining the appendages in absence of any torsion or ischemia.[2] Secondary epiploic appendagitis, on the other hand, develops due to inflammation of adjacent structures like appendicitis, diverticulitis or cholecystitis. PEA often presents with acute abdominal pain and can mimic acute diverticulitis or appendicitis on clinical examination. Its diagnosis is challenging due to the lack of any pathognomonic clinical features. Computed tomography (CT) scan has an important role in the diagnosis of PEA.[3] Timely diagnosis can avoid unnecessary surgical treatment.
Case report
A 35-year-old woman presented with sudden onset, severe pain abdomen since five days; localized to the upper left quadrant of the abdomen. The pain was accompanied by fever for initial two days. There was no history of constipation or vomiting. Physical examination revealed marked tenderness over the left upper quadrant of the abdomen with peritoneal sign of guarding and rebound tenderness. Rest of the physical examination was normal. All laboratory tests were within normal limits including white cell count, serum amylase, and liver and renal function tests. Pregnancy test was also negative.
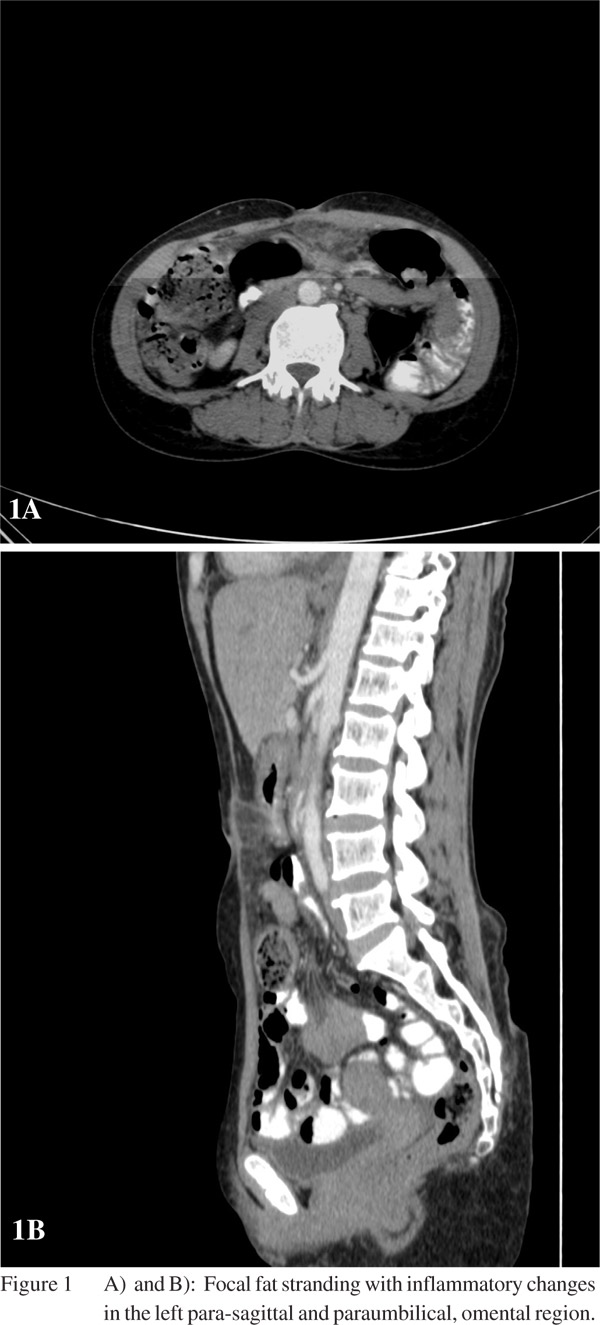
Ultrasound examination of the abdomen revealed a hyperechoic non-compressible pericolonic mass, and no organomegaly was seen. The persistent pain with localized peritoneal sign, prompted us to perform a contrast-enhanced CT scan of the abdomen and pelvis. The CT scan revealed focal fat stranding with mesenteric fat inflammation adjacent to the colon in the left para-sagittal, paraumbilical, omental region, which were consistent with the diagnosis of epiploic appendagitis (Figures 1A & 1B). Colonoscopic examination was normal. The patient was treated conservatively and she improved within a few days.
 Discussion
Discussion
Primary epiploic appendagitis is not as rare as is often thought. Its frequency is estimated at 1.3% in patients presenting with acute pain abdomen.[4] The main presenting symptom is severe, sudden onset, focal abdominal pain with localized tenderness and guarding. However, the symptoms tend to regress within a week. Omental infarct is another entity that has similar clinical and radiological characteristics, but on CT scan, omental infarct often presents as a much larger lesion with no visceral peritoneal thickening.[5,6] Pathognomonic CT scan finding of PEA is a 2–4 cm, oval shaped, fat density lesion, surrounded by inflammatory changes. In contrast to diverticulitis, the colon reveals a uniform diameter with a regular wall and no signs of thickening.[5,6] Given its self-limiting course with spontaneously resolution, patients with PEA are conservatively managed.[7] In conclusion, in a patient presenting with sharp, localized, acute abdominal pain unassociated with nausea, vomiting, fever or laboratory values typical of acute abdomen, a differential diagnosis of PEA should be entertained, and a CT scan abdomen should be performed to clinch the diagnosis.
References
- Desai HP, Tripodi J, Gold BM, Burakoff R. Infarction of an epiploic appendage. Review of the literature. J Clin Gastroenterol. 1993;16:323–5.
- Rioux M, Langis P. Primary epiploic appendagitis: clinical, US, and CT findings in 14 cases. Radiology. 1994;191:523–6.
- Macari M, Laks S, Hajdu C, Babb J. Caecal epiploic appendagitis: an unlikely occurrence. Clin Radiol. 2008;63:895–900.
- de Brito P, Gomez MA, Besson M, Scotto B, Huten N, Alison D. [Frequency and epidemiology of primary epiploic appendagitis on CT in adults with abdominal pain]. J Radiol. 2008;89:235–43.
- Rao PM, Wittenberg J, Lawrason JN. Primary epiploic appendagitis: evolutionary changes in CT appearance. Radiology. 1997;204:713–7.
- Pereira JM, Sirlin CB, Pinto PS, Jeffrey RB, Stella DL, Casola G. Disproportionate fat stranding: a helpful CT sign in patients with acute abdominal pain. Radio Graphics. 2004;24:703–15.
- Ghosh BC, Shatzkes J, Webb H. Primary epiploic appendagitis: diagnosis, management, and natural course of the disease. Mil Med. 2003;168:346–7.
|