|
|
|
|
 |
|
| |
 |
|
|
Case Report |
|
|
|
|
|
Keywords :
|
|
|
Arvind Ahuja1, Archna Rastogi1, Chaggan Bihari1, Yashwant Patidar2, Virendra Pamecha3, Shiv K Sarin4
Departments of Pathology,1 Radiology,2
Surgical Hepatology3 and Hepatology,4
Institute of Liver and Biliary Sciences,
New Delhi - 110070, India
Corresponding Author:
Dr. Arvind Ahuja
Email: drarvindahuja@gmail.com
DOI:
http://dx.doi.org/10.7869/tg.165
48uep6bbphidvals|668 48uep6bbph|2000F98CTab_Articles|Fulltext Hepatocellular carcinoma (HCC) is the sixth most common malignancy and the third most frequent cause of cancer mortality worldwide with increasing incidence both in developed and developing countries.[1] Although chronic viral hepatitis (B and C) and alcoholic liver disease (ALD) are the commonest and well established risk factors for HCC, there is now sufficient evidence and literature to suggest that nonalcohalic fatty liver disease (NAFLD) is also an important risk factor for the development of cirrhosis and may develop HCC.[2,3]
In addition to the already described histological variants of HCC, recently a new histological subtype has been described by Salomao et al.[4] This new variant was termed as steatohepatitic variant of hepatocellular carcinoma (SH-HCC), identified in liver explants with chronic hepatitis C. The histomorphological features of this variant resembled that of non-neoplastic steatohepatitis. The common findings described in this new variant include large droplet steatosis, inflammation, ballooning of malignant hepatocytes, Mallory- Denk bodies and pericellular fibrosis.[4,5] The same authors have shown that SH-HCC are strongly associated with underlying steatohepatitis and metabolic syndrome.[5] We could identify the first case of this new histological subtype of HCC out of 14 explant/resected liver specimens we received in 2 years duration.
Case report
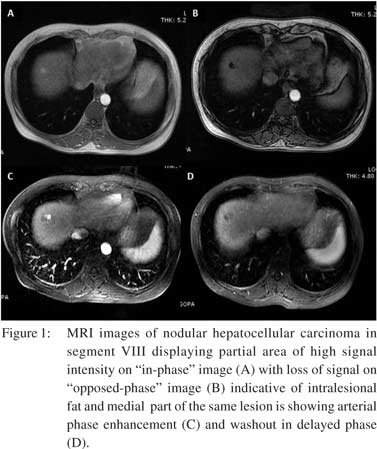
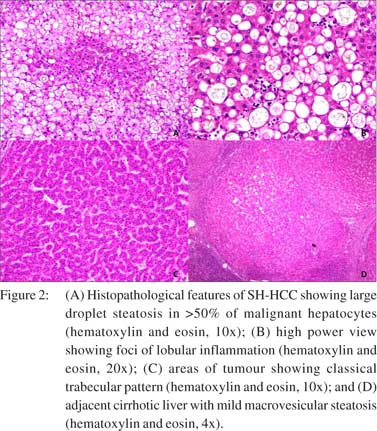
A 49-year- old female, a known case of hepatitis C related chronic liver disease was referred to the Hepatology out-patient department at our institute for evaluation and management. She was evaluated at our centre for chronic liver disease and investigated accordingly. Triple phase computerized tomography (CT) of abdomen showed changes of chronic liver disease with cirrhosis along with splenomegaly and multiple abdominal collaterals. On MRI there were three small 1 to 1.3 cm heterogeneous lobulated lesions seen in segment VIII, with arterial phase enhancement and washout in venous and delayed phase which were suggestive of HCC (Figure 1). Triple phase contrast enhanced (with Gadolinium BOPTA) multiplanar imaging of the upper abdomen also showed changes of chronic liver disease with cirrhosis and portal hypertension (splenomegaly and abdominal collaterals). Laboratory investigations showed total biliribin of 1.91 mg/dl, with a direct fraction of 0.68 mg/dl, aspartate aminotransferase level of 116 IU/L, alanine aminotransferase of 85 IU/L, lactate dehydrogenase of 75 IU/L, gamma glutamyl transferase of 47 IU/L, total protein of 7.1 g/dl with albumin level of 2.7 g/dl. She was detected to be diabetic with fasting glucose of 156 mg/dl and HbA1c 9.59. The HCV RNA levels were 1.76×105 IU/ml by real time PCR and the HCV virus belonged to the third genotype. Serum AFP level was 16.2 ng/ml. Her lipid profile was within normal range. According to Milano criteria for transplant in HCC, she was offered live donor liver transplant (LDLT); which she underwent. She is doing well after 2 months of LDLT. Histopathology examination of the liver explants showed distortion of the lobular architecture and formation of microand macro-nodules divided by thin fibrous septae. These septae showed mild chronic inflammation and lymphoid aggregates. Hepatocytes showed focal mild macrovesicular steatosis, focal ballooning and foci of lobular inflammation (Figure 2). Sections from the tumour nodules showed trabecular and solid pattern. The hepatocytes showed mild to
moderate nuclear pleomorphism and fair amount of cytoplasm, ballooning, large areas showing large droplet macrovesicular steatosis and many foci of lobular inflammation. Very occasional malignant hepatocyte showed Mallory’s hyalinelike material. The steatohepatitic morphology involved approx 70% of the tumour area. Silver reticulin stain revealed poor or absent staining in the tumour areas. In view of the characteristic morphological features a diagnosis of steatohepatitic variant of hepatocellular carcinoma was made.
Discussion
HCC is the most common primary malignant neoplasm of liver. It usually occurs in the setting of chronic liver disease and cirrhosis. Hepatic carcinogenesis is probably a multistep process that involves various risk factors, the commonest being chronic viral hepatitis (B and C), alcoholic liver disease (ALD), hemochromatosis, toxins and recently NAFLD. The incidence of HCC in USA is increasing possibly because HCV infection could have synergistic effect with risk factors like NAFLD, diabetes and metabolic syndrome.[6] Conventional HCC can show varied histological patterns such as trabecular, acinar, solid and scirrhous patterns. In addition, few variants of HCC have already been described in textbooks like the fibrolamellar variant and clear cell variant, based on identification of the characteristic histological features. However, recently a new variant termed SH-HCC has been described by Salomao et al, which can show all the patterns described above along with at least 3 steatohepatitis like features and steatohepatitic phenotype involving at least 50% of the tumour.[4,5] The steatohepatitis like features include large droplet steatosis, inflammation, ballooning of malignant hepatocytes, Mallory- Denk bodies and pericellular fibrosis within the neoplastic tissue. This variant was recognized in liver explants of patient with chronic hepatitis C related HCC and nearly all cases of SH-HCC were associated with underlying NASH or ALD. The same authors have also shown that this variant is strongly associated with metabolic syndrome.[5] The SH-HCC variant was found in a total of 22 of 62 HCC cases (35.5%) reported by Salomao et al in liver explants from patients with chronic hepatitis C. The main histological differentials of this variant include clear cell and steatotic subtype. The former shows polygonal cells with clear cytoplasm and the later shows presence of fat droplets in the cytoplasm. Inflammation, ballooning and pericellular fibrosis, the characteristic features of SH-HCC, are absent in both clear cell and steatotic subtypes. To conclude, we report the first case of SH-HCC variant from our centre and probably from India. This variant is mostly related to hepatitis C virus related chronic liver disease along
with a strong association with NASH or ALD. It shows distinct histopathological features which are usually not seen in conventional HCC. Recognition and documentation of this variant is important in context to the global epidemic of NAFLD/NASH and to further study the possible role of steatohepatitis in liver carcinogenesis.
References
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–917.
- Farrell GC, Larter CZ. Nonalcoholic fatty liver disease: from steatosis to cirrhosis. Hepatology. 2006;43:S99–S112.
- Hashimoto E, Yatsuji S, Tobari M, Taniai M, Torii N, Tokushige K, et al. Hepatocellular carcinoma in patients with nonalcoholic steatohepatitis. J Gastroenterol. 2009;44 Suppl 19:89–95.
- Salomao M, Yu WM, Brown RS, Jr., Emond JC, Lefkowitch JH. Steatohepatitic hepatocellular carcinoma (SH-HCC): a distinctive histological variant of HCC in hepatitis C virus-related cirrhosis with associated NAFLD/NASH. Am J Surg Pathol. 2010;34:1630–6.
- Salomao M, Remotti H, Vaughan R, Siegel AB, Lefkowitch JH, Moreira RK. The steatohepatitic variant of hepatocellular carcinoma and its association with underlying steatohepatitis. Hum Pathol. 2012;43:737–46.
- Davis GL, Alter MJ, El-Serag H, Poynard T, Jennings LW. Aging of hepatitis C virus (HCV)-infected persons in the United States: a multiple cohort model of HCV prevalence and disease progression. Gastroenterology. 2010;138:513–21, 21 e1–6.
|
|
|
|
|
|