|
|
|
|
 |
|
| |
 |
|
|
Original Articles |
|
|
|
|
|
Keywords :
Serum cholinesterase, decompensated cirrhosis, liver failure, compensated cirrhosis, biomarker, albumin |
|
|
Jeyamani Ramachandran,1 KG Sajith,1 Sophiya Priya,2 Amit K Dutta,1 KA Balasubramanian2
Division of G.I. Sciences,1
Wellcome Research Laboratory,2
Christian Medical College,
Vellore - 632004, India
Corresponding Author:
Dr. Jeyamani Ramachandran
Email: jeyapati@yahoo.com
DOI:
http://dx.doi.org/10.7869/tg.158
Abstract
Background: Serum cholinesterase (ChE) is an enzyme synthesised by hepatocytes and its serum levels reflect the synthetic function of liver .
Methods: In patients with cirrhosis, liver function tests, PT INR and serum ChE levels were done within a week of enrolment. We studied 178 cirrhosis patients and 154 healthy controls prospectively. Receiver operator characteristics (ROC) curve analysis was employed to compute an optimal cut-off level to distinguish these groups. Correlation between ChE activity and serum bilirubin, albumin, PT INR and MELD score (Model for End-Stage Liver Disease) was analysed.
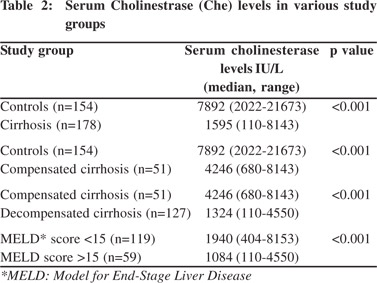
Results: Median serum ChE in cirrhotics was 1590 IU/L (110-8143) compared to controls 7886 IU/L (2022- 21673), p<0.001. Serum ChE levels below 3506 had a 98.7% sensitivity and 80.3% specificity in predicting cirrhosis. Median serum ChE was higher (p<0.001) in CC (n=51) 4246 IU/L (680-8143) compared to DC (n=127) 1324 IU/L (110-4550). ChE level less than 2385 IU/L had 80.1% sensitivity and 88.2% specificity in predicting DC. Follow-up levels in 25 patients showed good correlation with clinical course. The correlation coefficient between ChE and albumin was -0.67, 0.53 with PT INR and 0.59 with MELD score, (p<0.001).
Conclusions: Serum ChE is an excellent biomarker of cirrhosis with good sensitivity and specificity. It shows good correlation with serum albumin, PT INR and MELD score. Since it distinguishes DC from CC well, low levels in cirrhosis may serve as a useful prognostic marker of advanced liver disease. Long term follow-up studies are warranted to define its exact role in clinical practice.
|
48uep6bbphidvals|661 48uep6bbph|2000F98CTab_Articles|Fulltext Cholinesterases are enzymes classified by Mendel and Rudney into “true” cholinesterase or acetyl cholinesterase present in erythrocytes and glial tissues; and “pseudo” (succinyl or butryl or serum) cholinesterase, present in serum and synthesized in the liver.[1] Serum cholinesterase (ChE) appears to originate in the liver and is closely associated with the synthesis of serum albumin.[2,3,4] It has been shown that even very low pre-liver transplant serum cholinesterase levels improve by second week after a successful liver transplantation, thus confirming the hepatic origin of this enzyme.[5] Several workers as early as 1950s, have studied the value of serum cholinesterase estimation as a test of liver function, particularly to assess progress of chronic liver disease.[6] Subsequently, the prognostic value of ChE was evaluated by Hunt and Lehmann in predicting the outcome of portal venous shunt operations.[7]
Despite all the studies, this simple biochemical test is not routinely done as a liver function test worldwide. In this study, we evaluated serum ChE as a biomarker of cirrhosis by studying its levels in cirrhotics and controls. We also examined if serum ChE levels can differentiate decompensated cirrhosis (DC) from compensated cirrhosis (CC). We also examined for any correlation between ChE and other markers of liver function such as serum albumin.
Methods
This was a prospective study conducted after obtaining institutional ethics committee clearance. All study participants were enrolled after written informed consent. Consecutive cirrhotic patients of any etiology, referred to the outpatient liver clinic or admitted to inpatient hepatology services at our hospital from October 2010 to April 2011 were included in this study. Cirrhosis was proven by biopsy or ultrasonography (USG). Healthy volunteers with no clinical evidence of liver disease, including hospital staff and patients’ relatives were enrolled as controls after consent.
All cirrhosis patients were investigated for serum bilirubin, aspartate aminotransferase (AST), alanine aminotransferase, (ALT), total protein, albumin, PT INR, and serum ChE levels within a week of enrolment. The presence of DC was defined by the presence of either one or more of the following events; jaundice, variceal bleed, ascites requiring diuretics or paracentesis, hydrothorax, refractory ascites, spontaneous bacterial peritonitis, spontaneous bacterial empyema, encephalopathy and hepato-renal syndrome (HRS). Etiological evaluation consisted of viral markers, autoantibodies, serum ceruloplasmin and serum ferritin. The Model for End-Stage Liver Disease (MELD) score was calculated using the UNOS website.
Serum cholinesterase assay
The serum cholinesterase assay was carried out as described by Ellman et al using butyrylthiocholine iodide as substrate.8 The reagents, butyrylthiocholine iodide, eserine hemisulphate, and 5, 5’-dithio-bis (2-nitrobenzoic acid) were obtained from Sigma. Briefly the assay mixture contains 1.5 mM butrylthiocholine iodide (final concentration), 50µl of 1 M potassium phosphate buffer pH 7.0, 100 µl of 5, 5’-dithio-bis (2-nitrobenzoic acid) (DTNB) solution which contains 39.6 mg DTNB and 15 mg of sodium bicarbonate dissolved in 10 ml of 0.1 M phosphate buffer pH 7.0, serum sample 10 µl diluted 1 in 25 times with PBS. The volume of the assay was made up to 500 µl with deionised water and incubated for 10 minutes at 37°C. After incubation, butylcholinesterase (BChE) was inhibited by 0.25 mM eserine hemisulphate (final concentration) with the final volume made up to 1 ml. Product formation was determined at 412 nm under standard assay conditions. One unit of BChE corresponds to the enzyme required to hydrolyse 1 µmol of substrate into product per minute.
Serum ChE levels were compared between 1) the entire study cohort (cirrhotics) and controls and 2) between controls and patients with only compensated cirrhosis (CC), 3) between patients with compensated cirrhosis and decompensated cirrhosis and between 4) cirrhotic patients with MELD cut off 15. In addition, ChE levels were also correlated with serum bilirubin, albumin, PT INR and MELD score.
Statistical analysis
Comparison of serum ChE levels between the various groups was done using Mann-Whitney’s U test. Receiver operating characteristics (ROC) curves were computed to determine optimal serum ChE cut-off levels for differentiating different patient groups from each other. To evaluate correlations between serum ChE levels and other liver tests, Spearman’s correlation test was used. Data were analysed using SPSS v16. A p value <0.05 was considered significant.
Results
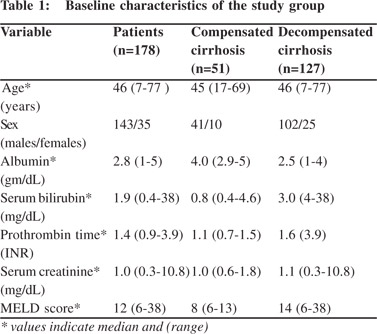
A total of 178 cirrhotic patients (35 women, 143 men) were studied .Their median age was 46 years (7-77 years). The etiology of liver disease was alcohol in 51, alcohol and hepatitis B or hepatitis C in 6, hepatitis B alone in 35, hepatitis C alone in 12, cryptogenic liver disease in 54, autoimmune in 9, miscellaneous (Wilson’s disease, secondary biliary cirrhosis and Budd-Chiari syndrome) in 11 patients. The diagnosis of cirrhosis was made by biopsy in 22 patients and USG in all. We enrolled 154 controls (53 women,101 men). Baseline details are described in Table 1. Among cirrhosis patients, 51 (28.7%) were in Child’s class A, labelled as compensated cirrhosis (CC), 46 (25.8%) were in Child’s class B and 81 (45.5%) were in Child’s class C. Child’s class B and C were labelled as decompensated cirrhosis (DC).
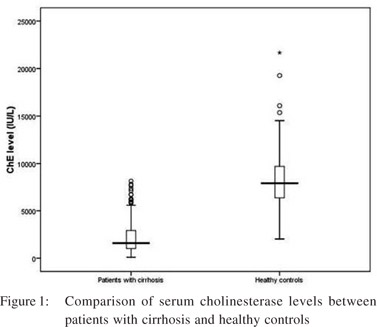
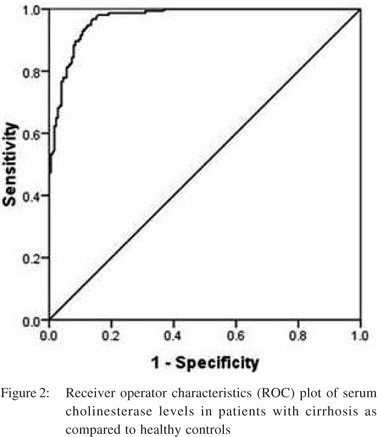
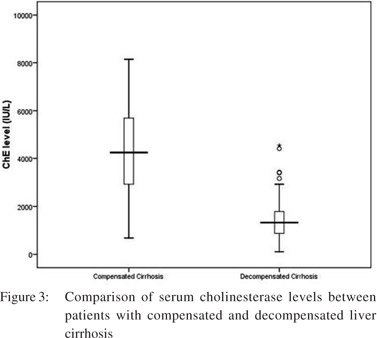
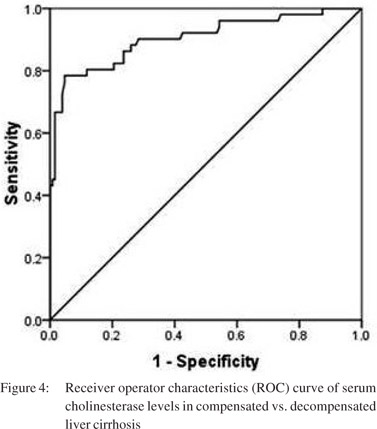
 Serum ChE levels in cirrhotics ranged from 110 to 8143 IU/L, with a median of 1590 IU/L. In healthy controls, the median ChE level was 7892 IU/L (2022-21673 IU/L).The difference between the two groups was significant (Figure 1) (Table 2). The ROC curve analysis to determine a predictive ChE cut-off level for cirrhosis yielded ChE levels below 3506 IU/L offered 98.7% sensitivity and 80.3% specificity for the diagnosis, with an area under the curve (AUC) of 0.97 (95% CI: 0.954-0.984, p<0.001) (Figure 2). The median ChE level in the CC group was 4246 IU/L (680-8143 IU/L) and in DC group was 1324 IU/L (110-4550 IU/L). The difference was statistically significant (p<0.01) (Figure 3). Serum ChE levels below 1800 IU/L, had a 80% sensitivity and 80% specificity for predicting DC (area under ROC curve=0.9, 95% CI: 0.848-0.961) (Figure 4). Thirty nine out of the 127 patients with DC had septic complications like spontaneous bacterial peritonitis, spontaneous bacterial empyema, septicaemia, cellulitis, and pneumonia. There was no significant difference in serum ChE levels between DC patients with or without active infection (1242 IU/L vs. 1360 IU/L, p =0.42). Twenty one patients presented with variceal bleed. There was no statistical difference in serum ChE levels between patients with and without variceal bleeds (1452 IU/L vs. 1599 IU/L, p=0.8).
Serum ChE levels in cirrhotics ranged from 110 to 8143 IU/L, with a median of 1590 IU/L. In healthy controls, the median ChE level was 7892 IU/L (2022-21673 IU/L).The difference between the two groups was significant (Figure 1) (Table 2). The ROC curve analysis to determine a predictive ChE cut-off level for cirrhosis yielded ChE levels below 3506 IU/L offered 98.7% sensitivity and 80.3% specificity for the diagnosis, with an area under the curve (AUC) of 0.97 (95% CI: 0.954-0.984, p<0.001) (Figure 2). The median ChE level in the CC group was 4246 IU/L (680-8143 IU/L) and in DC group was 1324 IU/L (110-4550 IU/L). The difference was statistically significant (p<0.01) (Figure 3). Serum ChE levels below 1800 IU/L, had a 80% sensitivity and 80% specificity for predicting DC (area under ROC curve=0.9, 95% CI: 0.848-0.961) (Figure 4). Thirty nine out of the 127 patients with DC had septic complications like spontaneous bacterial peritonitis, spontaneous bacterial empyema, septicaemia, cellulitis, and pneumonia. There was no significant difference in serum ChE levels between DC patients with or without active infection (1242 IU/L vs. 1360 IU/L, p =0.42). Twenty one patients presented with variceal bleed. There was no statistical difference in serum ChE levels between patients with and without variceal bleeds (1452 IU/L vs. 1599 IU/L, p=0.8).
Serum ChE as a predictor of MELD
The study patients were divided into two groups based on the MELD cut-off of 15. Serum ChE predicted high MELD status at a cut-off of 1484 IU/L, with 71% sensitivity and 73% specificity, and AUC of 0.77 (95% CI: 0.70-0.84) (Table 2). We further assessed the performance of serum ChE in comparison to other routine liver function tests. The correlation coefficients were as follows: 0.67 with serum albumin (p <0.01); 0.59 with MELD score (p<0.01); 0.53 with PT INR (p<0.01); and 0.47 with serum bilirubin (p<0.01).
Follow-up data was available for 25 patients, collected within 1-6 months after the initial enrolment. Depending on the clinical outcome we classified the patients into worsened (n=6), improved (n=7) and stable (n=12). Among those who clinically worsened, 5/6 had reduction in ChE levels (median: 680 IU/L. range: 222- 993 IU/L). In one patient there were more than one value showing a serial decline in serum ChE correlating with the downhill clinical course. Four out of these five patients died within three months of follow-up. One patient who improved six months later (from DC to CC) had serial elevation in serum ChE levels to the range seen in CC. Seven patients, whose clinical condition had significantly improved from DC to CC, showed an improvement in their ChE levels (median: 1719; range: 625-7757 IU/L) as well. Similarly, the patients whose clinical condition was stable and were in CC, had either similar levels or witnessed an increase in their serum ChE levels but no reduction.
Discussion
Serum ChE is unique in being exclusively synthesised by the liver like albumin and coagulation factors and thus its level is expected to decline in patients with cirrhosis. Several other studies have examined the utility of serum ChE levels as a possible liver function test, but have yielded equivocal conclusions.[2-4,6,7] Majority of these studies examined liver tumours or obstructive jaundice, conditions irrelevant today given the advancements in imaging modalities. Furthermore, new calorimetric techniques with more selective reagents have made the measurement of serum ChE very simple. This study was an attempt to evaluate and prove the utility of serum ChE as a biomarker of cirrhosis.
We found cirrhotics to have significantly lower levels of serum ChE as compared to healthy controls. We also found that patients with decompensated cirrhosis had significantly lower levels compared to well compensated cirrhosis. Even after stratifying the severity of liver disease by MELD scores , the difference remained significant. Presence of severe infection or variceal bleed did not confound the results. Serum levels of ChE showed excellent correlation with albumin and reasonably good correlation with serum bilirubin and PT INR which indicate that ChE levels reflect the functional integrity of liver.
Serum ChE levels have been shown to reflect liver function adequacy in various clinical situations.[9] For example in familial intrahepatic cholestasis, following successful external biliary diversion, increasing levels of serum ChE have been shown to be a marker of successful surgery.[10] Li Q et al have shown that in cases of severe chronic hepatitis, serum cholinesterase levels were found to be very low and were associated with increased mortality. The authors have suggested a logistic regression model employing serum ChE with better prognostic value than MELD.[11] Since serum ChE gives substantial information about the functional reserve of liver, it can be useful when deciding on incidental non-liver surgery, hepatic resection or transjugular intrahepatic portosystemic shunt (TIPS) in cirrhotic patients. Serum ChE measurement is much simpler than the cumbersome quantitative liver function tests. A new liver score, including serum ChE, albumin and bilirubin has been proposed for predicting postoperative hepatic dysfunction and outcome in cardiac patients with liver dysfunction.[12] A prognostic model employing serum albumin, size of the varices and serum ChE was found to be superior to Child’s score in predicting 1-, 3- and 5-year mortality in a cohort of alcoholic cirrhosis.[13]
It has also been shown that although normal levels of ChE activity vary widely, each individual retains his/her own level of serum ChE under normal circumstances.[9] Low levels in a cirrhotic patient need to be followed up and if persistently low, may be considered as yet another prognostic marker of advanced liver disease. Improving levels can be used to assess response in a cost effective way, as in specific therapy for cirrhosis such as antiviral treatment for hepatitis B, steroids for autoimmune hepatitis or chelation therapy in Wilson’s disease. Our follow-up though small, shows the potential role of this test in conditions such as ACLF where serial monitoring is essential to predict the course of liver disease. Crucial decisions such as need for liver transplantation may be guided by this test during follow-up. When we look at the contribution of this test in the diagnosis and prognosis of cirrhosis, there are a few points of merit. Serum ChE is a single biochemical test that can be easily made available. It can be repeated as often as required. In therapeutically anticoagulated patients such as those with Budd Chairi syndrome , PT INR is an unreliable marker of hepatic function. Similarly in patients receiving albumin supplements, which is very common in refractory ascites and type 2 HRS, the true synthetic function of the liver is masked but can be easily assessed by monitoring serum ChE. It can thus play an important role as a marker of liver function in circumstances where PT INR and serum albumin cannot be used. Ogunkeye et al suggested that serum ChE is a cost-effective diagnostic marker for differentiating between overt liver disease and nonhepatic diseases, where one may witness false aberrations in liver function tests.[14] In patients with coexistent renal disease, where serum creatinine is elevated independent of liver disease, the MELD score cannot be used to predict the severity of liver disease. However, this potential role of serum ChE needs to be studied in a well planned trial before drawing any conclusions. Similarly, more longitudinal studies are warranted examining the use of serum ChE in organ allocation in special situations with low MELD scores like refractory ascites. Serial follow-up in ACLF can help provide critical information about liver function recovery. It must however be remembered that in addition to liver disease, low serum ChE levels are also associated with chronic anemia, malignancy, severe acute infections, cardiac failure, burns and radiotherapy.[15]
In conclusion, serum ChE is an excellent biomarker of cirrhosis with good sensitivity and specificity. It shows good correlation with serum albumin, PT INR and the MELD score. Since it discriminates well between DC and CC, low levels in cirrhosis may be considered as yet another prognostic marker of advanced liver disease. Long term follow-up studies are warranted to define its exact role in clinical practice.
Acknowledgements.
The work was supported by institutional research grant provided by Christian Medical College, Vellore, India.
References
- Mendel B, Rudney H. Studies on cholinesterase: 1. Cholinesterase and pseudo-cholinesterase. Biochem J. 1943;37:59–63.
- Faber M. The relationship between serum cholinesterase and serum albumin. Acta med Scand. 1943;114:72.
- Kunkel HG, Ward SM. Plasma Esterase Activity in Patients with Liver Disease and the Nephrotic Syndrome. J Exp Med. 1947;86:325–37.
- Svensmark O. Enzymatic and Molecular Properties of Cholinesterases in Human Liver. Acta Physiol Scand. 1963;59:378–89.
- Aldrete JA, O’Higgins JW, Holmes J. Changes of plasma cholinesterase activity during orthotopic liver transplantation in man. Transplantation. 1977;23:404–6.
- Vorhaus LJ, Scudamore HH, Kark RM. Measurement of serum cholinesterase activity in the study of diseases of the liver and biliary system. Gastroenterology. 1950;15:304–15.
- Hunt AH, Lehmann H. Serum albumin, pseudocholine-sterase, and transaminases in the assessment of liver function before and after venous shunt operations. Gut. 1960;1:303–11.
- Ellman GL, Courtney KD, Andres V, Jr., Feather-Stone RM. A new and rapid colorimetric determination of acetylcholinesterase activity. Biochem Pharmacol. 1961;7:88–95.
- McQueen MJ. Clinical and analytical considerations in the utilization of cholinesterase measurements. Clin Chim Acta. 1995;237:91–105.
- Melter M, Rodeck B, Kardorff R, Hoyer PF, Petersen C, Ballauff A, et al. Progressive familial intrahepatic cholestasis: partial biliary diversion normalizes serum lpids and improves growth in noncirrhotic patients. Am J Gastroenterol. 2000;95:3522–8.
- Li Q, Yuan GY, Tang KC, Liu GW, Wang R, Cao WK. Prognostic factors for chronic severe hepatitis and construction of a prognostic model. Hepatobiliary Pancreat Dis Int. 2008;7:40–4.
- Nishi H, Takahashi T, Ichikawa H, Matsumiya G, Matsuda H, Sawa Y. Prediction of postoperative hepatic dysfunction after cardiac surgery in patients with chronic congestive heart failure. Gen Thorac Cardiovasc Surg. 2009;57:357–62.
- Zimmerer J, Haubitz I, Mainos D, Hadass H, Tittor W. Survival in alcoholic liver cirrhosis: prognostic value of portal pressure, size of esophageal varices and biochemical data. Comparison with Child classification. Z Gastroenterol. 1996;34:421–7.
- Ogunkeye OO, Roluga AI. Serum cholinesterase activity helps to distinguish between liver disease and non-liver disease aberration in liver function tests. Pathophysiology. 2006;13:91–3.
- Robertson GS. Serum cholinesterase deficiency. I. Disease and inheritance. Br J Anaesth. 1966;38:355–60.
|
|
|
|
|
|