48uep6bbphidvals|616
48uep6bbph|2000F98CTab_Articles|Fulltext
We report a rare case of management of metastatic carcinoma colon with postoperative recurrence in a patient who had presented with anastomotic stricture and acute intestinal obstruction. She underwent combined percutaneous fluoroscopic insertion of guidewire and rendezvous insertion of fully covered self-expanding metallic stent (SEMS) and achieved palliation.
Case report
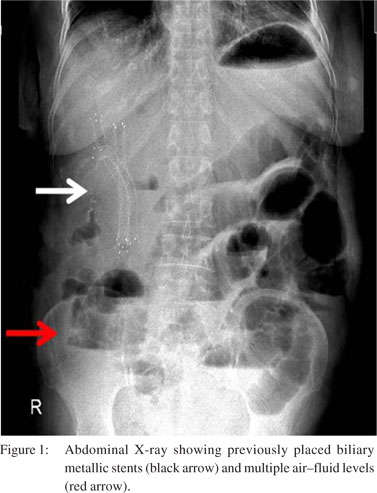
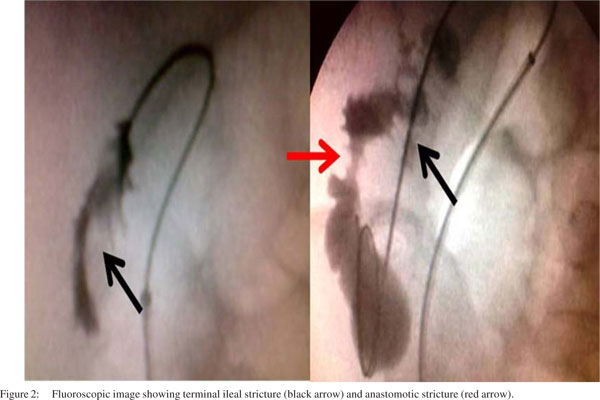
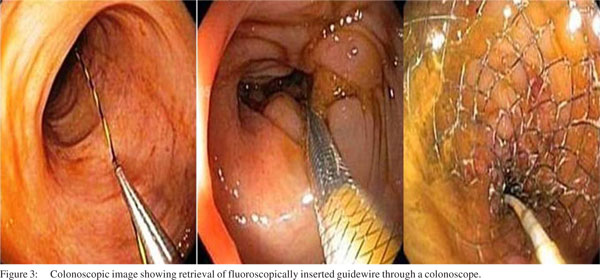
A 67-year-old woman, a known case of carcinoma colon (postright hemicolectomy), presented with a history of jaundice for the past 6 months due to lymph node metastases at the porta hepatis. Percutaneous stenting (Luminexx Bard) of the right anterior, right posterior and left biliary system was done (as endoscopic retrograde cholangiopancreatigraphy failed) to palliate jaundice. No further treatment was opted because of her poor performance status. The patient was largely aymptomatic for 6 months after which she presented with acute intestinal obstruction (Figure 1) due to recurrence of tumour at the anastomotic site. After initial resuscitation, stenting was attempted to relieve obstruction using colonoscopy. However, guidewire could not be negotiated across the site of anastomotic stricture. As the patient was moribund and the success of spiral enteroscopy-assisted SEMS deployment was questionable due to terminal ileal location of the stricture;[1] the rendezvous technique was preferred over other methods. Computed tomography (CT) scan-assisted percutaneous access of the ileal loop was achieved just proximal to the obstruction followed by delineation of stricture details with contrast under fluoroscopic guidance. Fluoroscopy showed two strictures—one at the terminal ileum and the other at the anastomotic site (Figure 2). Guidewire was inserted percutaneously and negotiated across the strictures. It was pulled through the colonoscope followed by placement of two stents (Bona stent, Standard Sci-Tech, Seoul, Korea)—first at the anastomotic site and the second at the terminal ileum (Figure 3). Subsequently, the small bowel was decompressed (Figure 4) and the patient improved. The patient is asymptomatic after 3 months of follow-up.
 This case is an illustration of successful palliation of malignant enteral strictures using the rendezvous stent insertion technique in patients with poor surgical risk.
Reference
This case is an illustration of successful palliation of malignant enteral strictures using the rendezvous stent insertion technique in patients with poor surgical risk.
Reference
- Lennon AM, Chandrasekhara V, Shin EJ, Okolo Pi 3rd. Spiralenteroscopy- assisted enteral stent placement for palliation of malignant small-bowel obstruction (with video). Gastrointest Endosc. 2010;71:422–5.