|
|
|
|
 |
|
| |
 |
|
|
Case Report |
|
|
|
|
|
Keywords :
|
|
|
UC Singh1, Ashok Kumar1, Anil Srivastava1, Brijesh Patel1, VK Shukla2, SK Gupta2
Department of Surgery,1
BRD Medical College, Goarakhpur,
Institute of Medical Sciences, BHU, Varanasi,2
Uttar Pradesh, India
Corresponding Author:
Dr. UC Singh
Email: drucsinghbhu@yahoo.in
DOI:
http://dx.doi.org/
48uep6bbphidvals|473 48uep6bbph|2000F98CTab_Articles|Fulltext Fasciolopsis buski infestation is not a new entrant in the list of parasitic diseases[1] prevalent in Southeast Asia including southern and central China, Vietnam, Thailand, Laos, Taiwan,Bangladesh, Indonesia and India.[2,3,4,5,6] In India cases have been mostly reported from eastern U.P., Bengal and Biharprovinces.[7,8,9,10] This infestation is prevalent in areas where water plants such as water chestnut (“shingara” or Trapa bicornis), water caltrops and water bamboo are cultivated and inhabitants consume contaminated water and uncooked water plants. This is the first case report of this parasitic infestation in literature, giving rise to multiple strictures and perforation of small bowel and the first such report from an institution situated in the same geographical area. As this problem is a public health concern, an awareness regarding its disease severity is required for prompt patient management.
Case Report
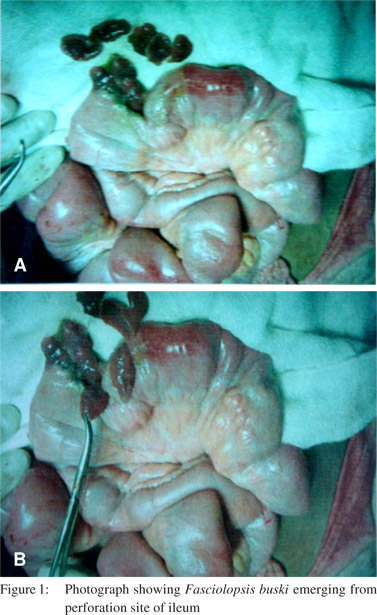
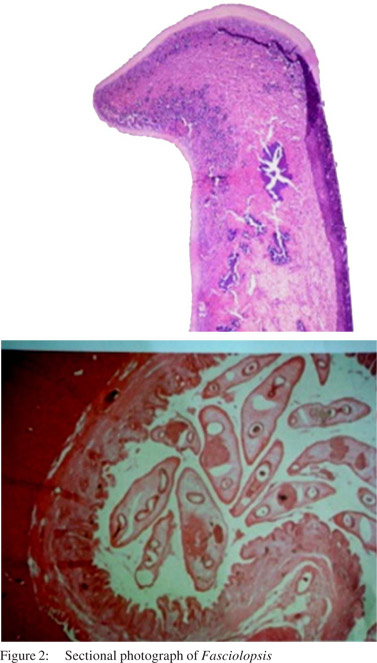
A female patient aged about 22 years from a district of eastern U.P., India was admitted in the surgical emergency of BRD Medical College, Gorakhpur, U.P., with complaints of absolute constipation, abdominal distension, fever and vomiting for 4-5 days. On physical examination she was toxic, febrile, anemic, dehydrated, tachypneic, and had tachycardia. Abdominal examination revealed features of peritonitis. Plain erect X-ray abdomen showed gas under right dome of diaphragm. Blood biochemistry revealed hemoglobin of 8 gm/dl, leucocytosis with the following differential count: polymorphs 84%, lymphocytes 10% and monocytes 6%. Renal biochemical profile revealed a serum urea of 54.2 mg/dl and serum creatinine of 1.39 mg/dl. Her blood sugar was 168 mg/dl and there was no dyselectrolytemia. Serum amylase was normal. After resuscitation she underwent an emergency exploratory laparotomy. On opening the peritoneum large amount of purulent fluid was found along with a number of liver flukes which were floating in the fluid. The fluid was sucked out and the viscera were examined. There were two strictures in the ileum, the first one was 2 feet distal to the duodenojejunal flexure and the distal one was 1.5 feet proximal to ileocolic junction. There was a large perforation over the distal strictured bowel segment. Other abdominal viscera including the liver were normal. We resected the proximal strictured bowel and a large number of liver flukes came out from lumen (Figure 1). By milking the proximal bowel we removed as many liver flukes as possible. An end to end anastomosis of the bowel was performed. The distal strictured segment along with the perforation was also resected and a double barrel ileostomy was performed. Histopathological examinations of the specimen showed presence of Fasciolopsis buski (Figure 2). After thorough peritoneal lavage, a suction drain was kept in the pelvis and abdomen was closed in layers. She was shifted to emergency ward but developed postoperative hypoxia and unstable blood pressure for which she was shifted to the intensive care unit (ICU). She made a rapid recovery and was discharged from the ICU and shifted to the general surgery ward on the 4th day. Subsequently she was allowed oral feeds from the 6th post operative day. On 8th post operative day oral Praziquantel (25 mg/kg) was given in divided doses for one day. Few liver flukes were also recovered from the ileostomy bag during hospitalization.[11] She was discharged from the hospital on day 14 as the remaining post-operative period was unremarkable. She was readmitted after 3 months for closure of the stoma. She recovered completely. During follow up her stool was negative for ova of Fasciolopsis buski.
Discussion
The adult worm of Fasciolopsis buski normally inhabits the duodenal and jejunal mucosa in mild to moderate infestation, but it can be found anywhere from the stomach to the colon in heavy infestation. Eggs are liberated in faeces of infected animals (pigs and dogs)[12] and human beings. Liberated eggs get encysted as metacercariae which is an infective stage for human and other definitive hosts after passing through the intermediate host found in fresh water plants. The clinical manifestation depends on parasitic load in gut, local pathological changes and absorption of toxic allergic metabolites. Patient may be asymptomatic or may present with various symptoms like abdominal pain, diarrhea, poor appetite and vomiting. Some patients may present with features of intestinal obstruction or perforation whereas a small group of patients may present with anasarca and even succumb to the illness.3-5 After consideration of such a huge worm load, it can be inferred that she had consumed large numbers of metacercariae over a prolong period as there is no multiplication of the parasite in the definitive host. The inhabitants are familiar with the worm and call it “Petari” in local language, and despite that there is paucity of preventive measures and health education in this endemic area.[13] A heavy infestation of these parasites can cause ulceration, abscess and haemorrhage in the ileum which can give rise to strictures and perforation[14] over strictured segments. This was further proved by histopathological examination of the strictured bowel segment in the present case, which revealed nonspecific chronic inflammation and submucosal fibrosis and dilated lymphatics. There was no evidence of granuloma or atypia and rest of the mucosa was unremarkable.
Such a serious presentation of Fasciolopsis buski has not been reported in the past. Therefore it can be added in the list of causes of small bowel strictures as a rare possibility in patients from endemic areas. This in turn can help in the diagnosis and management. Health authorities should initiate appropriate preventive and awareness measures in these areas, considering the serious course of this disease. Furthermore such measures will be important for continuing medical education of medical personnel working in these endemic areas and to sensitize them to current issues of public health.
References
- Shah A, Gagdil RK, Manohar KD. Fasciolopsiasis in Bombay. Ind J Med Sci. 1966;20:805–11.
- Wiwanitkit V ,Suwanasksi J ,Chaiyakhun Y. High prevalence of Fasciolopsis buski in an endemic area of liver fluke infection in Thailand. Med Gen Med. 2002;4:6.
- Lo CT, Lee KM. Intestinal parasites among the Southeast Asian laborers in Taiwan during 1993-1994. Zhonghua Yi Xue ZA Zni (Taipei ). 1996;57:401–4.
- Gilman RH ,Mondal G, Maksud M, Alam K, Rutherford E, Gilman JB, et al. Endemic focus of Fasciolopsis buski infection in Bangladesh. Am J Trop Med Hyg. 1982;31:796–802.
- Le TH ,Nguyen VD ,Phan BU ,Blair D ,Mc Manus DP. Case report: unusual presentation of Fasciolopsis buski in a Vietnamese child. Trans R Soc Trop Med Hyg. 2004;98:193–4.
- Yu S, Xu L, Jiang Z, Xu S, Han J, Zhu Y, et al. Report on the first nationwide survey of the distribution of human parasites in China. 1. Regional distribution of parasite species. Zhongguo Ji Sheng Chong Xue Yu Ji Sheng Chong Bing Za Zhi. 1994;12:241–7.
- Kumari N ,Kumar M ,Rai A ,Acharya A. Intestinal trematode infection in North Bihar. JNMA J Nepal Med Assoc. 2006;45:204–6.
- Gupta A, Xess A, Sharma HP, Dayal VM, Prasad KM, Shahi SK. Fasciolopsis buski (giant intestinal fluke)— a case report. Indian J Pathol Microbiol. 1999;42:359–60.
- Muralidhar S, Srivastava L, Aggarwal A, Jain N, Sharma DK. Fasciolopsiasis--a persisting problem in Eastern U.P.—A case report. Indian J Pathol Microbiol. 2000;43:69–71.
- Bhatti HS ,Malla N ,Mahajan RC ,Sehgal R. Fasciolopsiasis—re emerging infection in Azamgarh (Uttar Pradesh). Indian J Pathol Microbiol. 2000;43:73–6.
- Mahajan RK, Duggal S, Biswas NK, Duggal N, Hans C. A finding of live Fasciolopsis buski in an ileostomy opening. J Infect Dev Ctries. 2010;4:401–3 .
- Roy B, Tandan V. Seasonal prevalence of some zoonotic trematode infections in cattle and pigs in north-east zone in India. Vet Parasitol. 1990;41:69–76.
- CD Alert. Food borne tremtode (Fluke ) infections. A neglected health problem in India. November 2005 ,Vol. 9 no. 11.
- Battacharjee HK ,Yadav D, Bagga D. Fasciolopsiasis presenting as intestinal perforation: a case report. Trop Gastroenterol. 2009;30:40–1.
|
|
|
|
|
|